The Effects of Traction and Vacuum-Based Therapies on Non-Surgical Penis Enlargement: A Prospective Cohort Study
2025 Apr 28.
McKringlebry, Hinkle ¹
AKA “The Hink Trial”
Intro
Concerns regarding penile size have persisted across cultures since ancient times, reflecting the longstanding psychological and sociocultural significance of this physical attribute. In the modern era, the proliferation of pornography and social media has intensified these insecurities, fueling a global increase in the demand for penile enhancement procedures. Many of these interventions, including high risk surgeries and injectable fillers, carry substantial morbidity, as highlighted by Moore et al. (2024).
Non-surgical methods have emerged as alternatives, with studies by Nikoobakht et al. (2011) and Nowroozi et al. (2015) demonstrating that penile traction therapy can achieve mean length gains of up to 2 cm. The P-Long Study by Brandeis et al. (2023) further reported combined length and girth increases through the use of traction devices, vacuum erection therapy, and platelet-rich plasma injections. However, the lack of objective photographic verification across these trials undermines the reliability of the reported outcomes, and no prior study has demonstrated girth enhancement through fully noninvasive means.
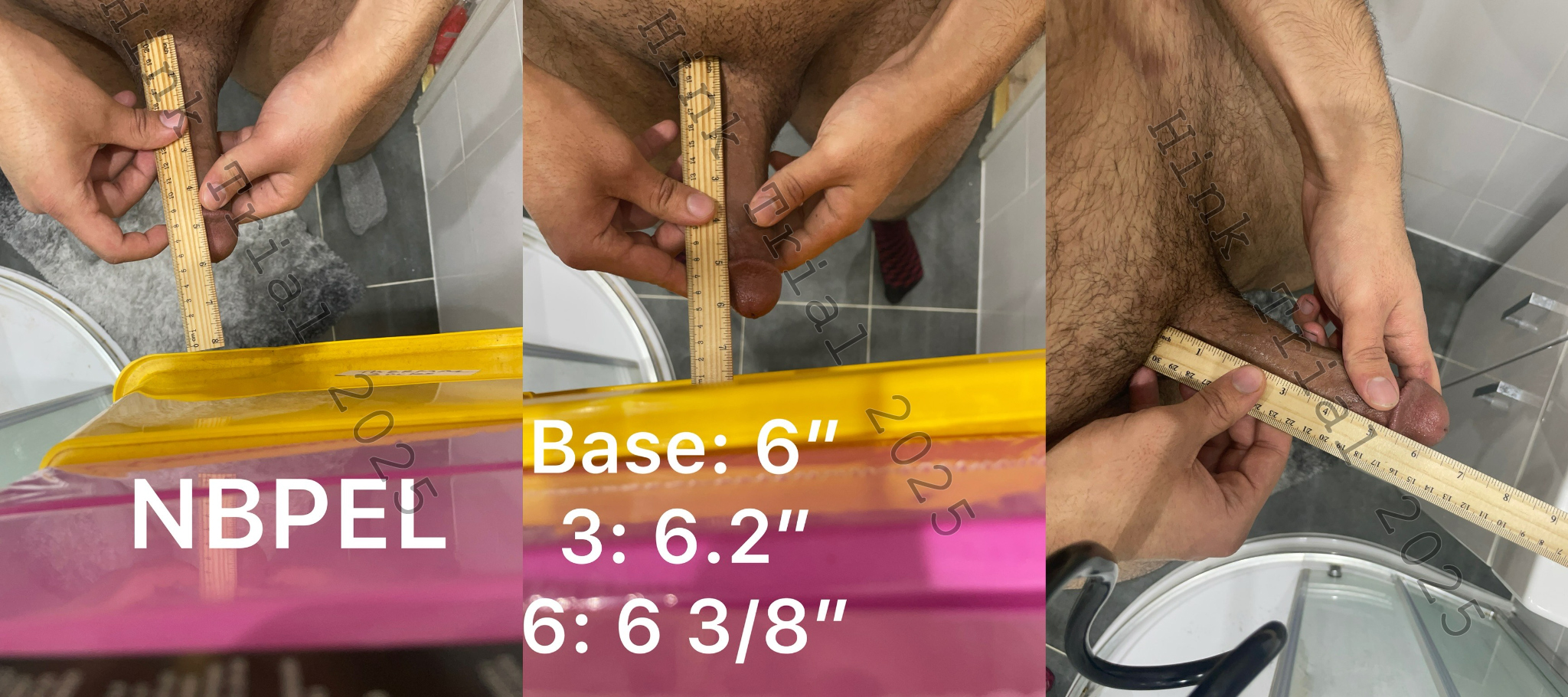
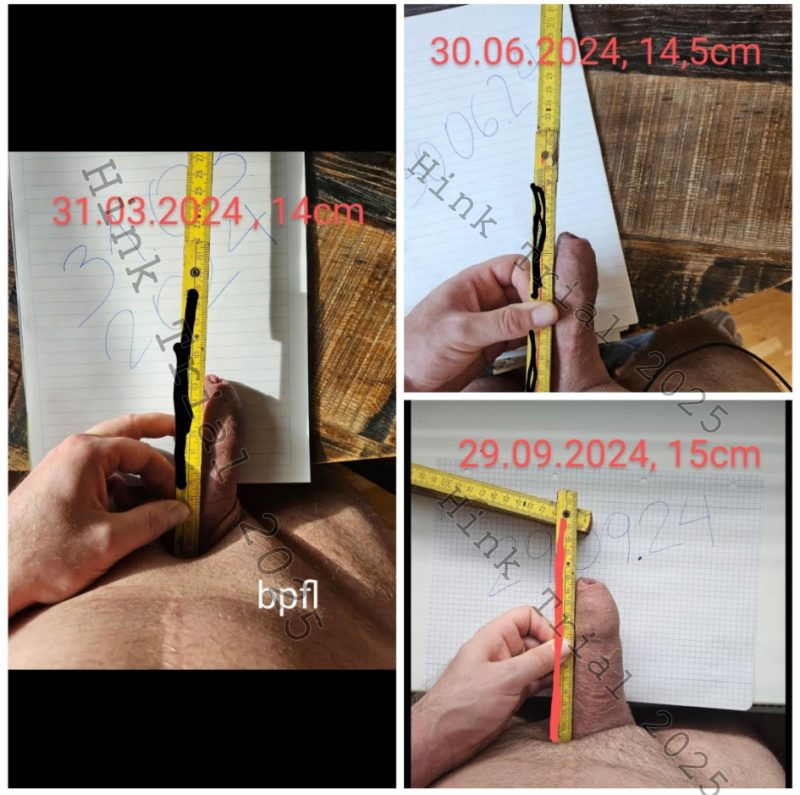
This study, titled “The Hink Trial,” was designed to address these limitations by providing the first systematic evaluation of non-surgical penile enhancement verified through standardized photographic documentation. It aims to demonstrate that significant increases in penile length and girth can be achieved without the need for invasive procedures or substantial financial burden.
Methods
Eligible participants were healthy males aged 20 to 64 years, without a prior diagnosis of erectile dysfunction or other significant medical comorbidities. Inclusion was further restricted to individuals with limited or no previous experience with penile enlargement techniques. Participants were self-referred and voluntarily enrolled in response to recruitment advertisements posted on the online forums r/gettingbigger and r/hink.
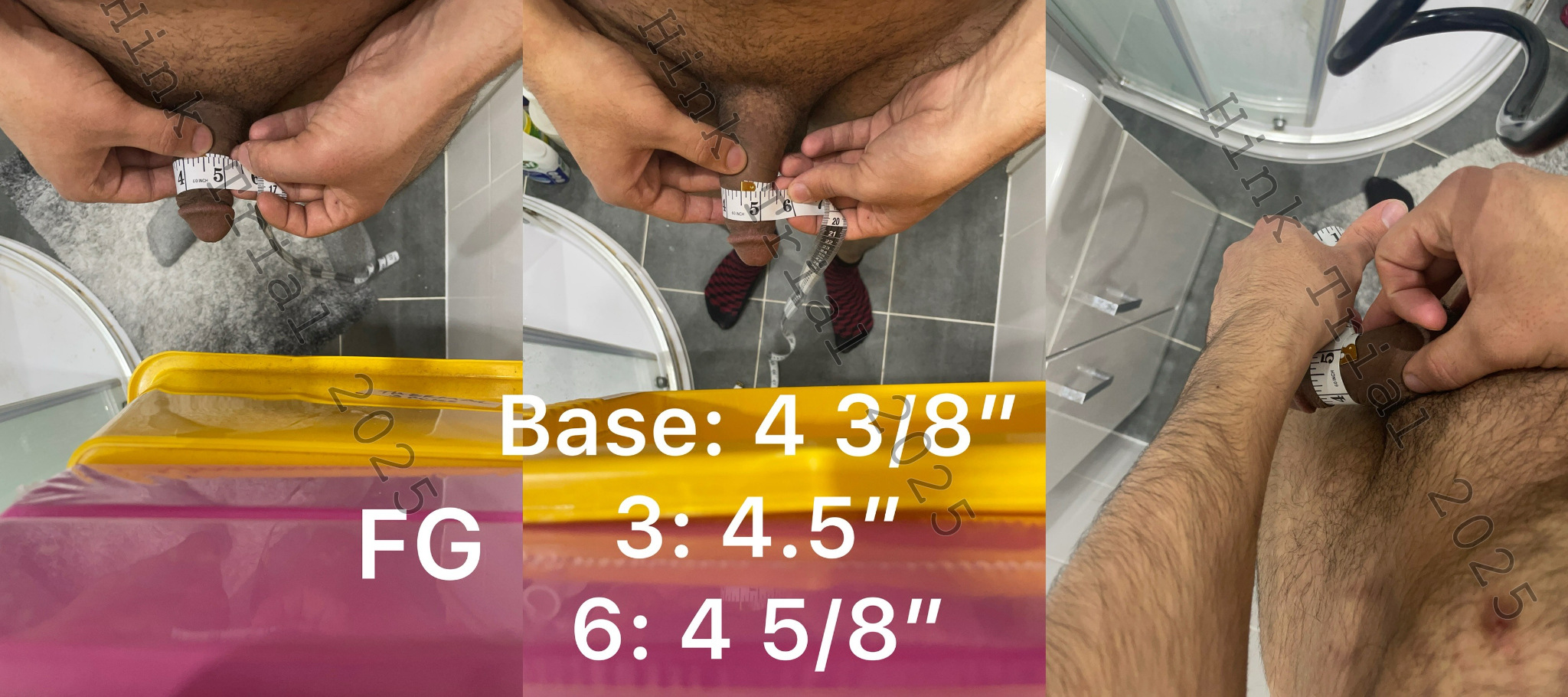
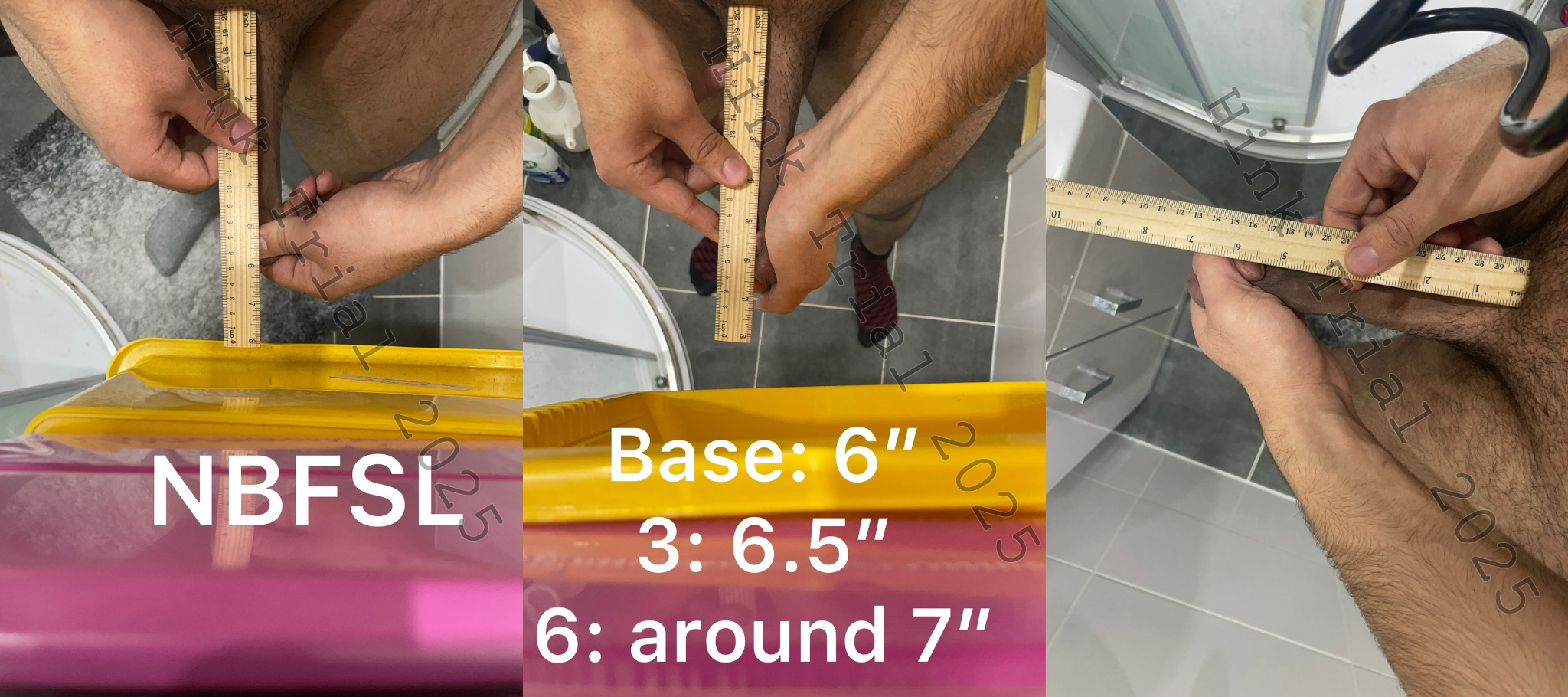
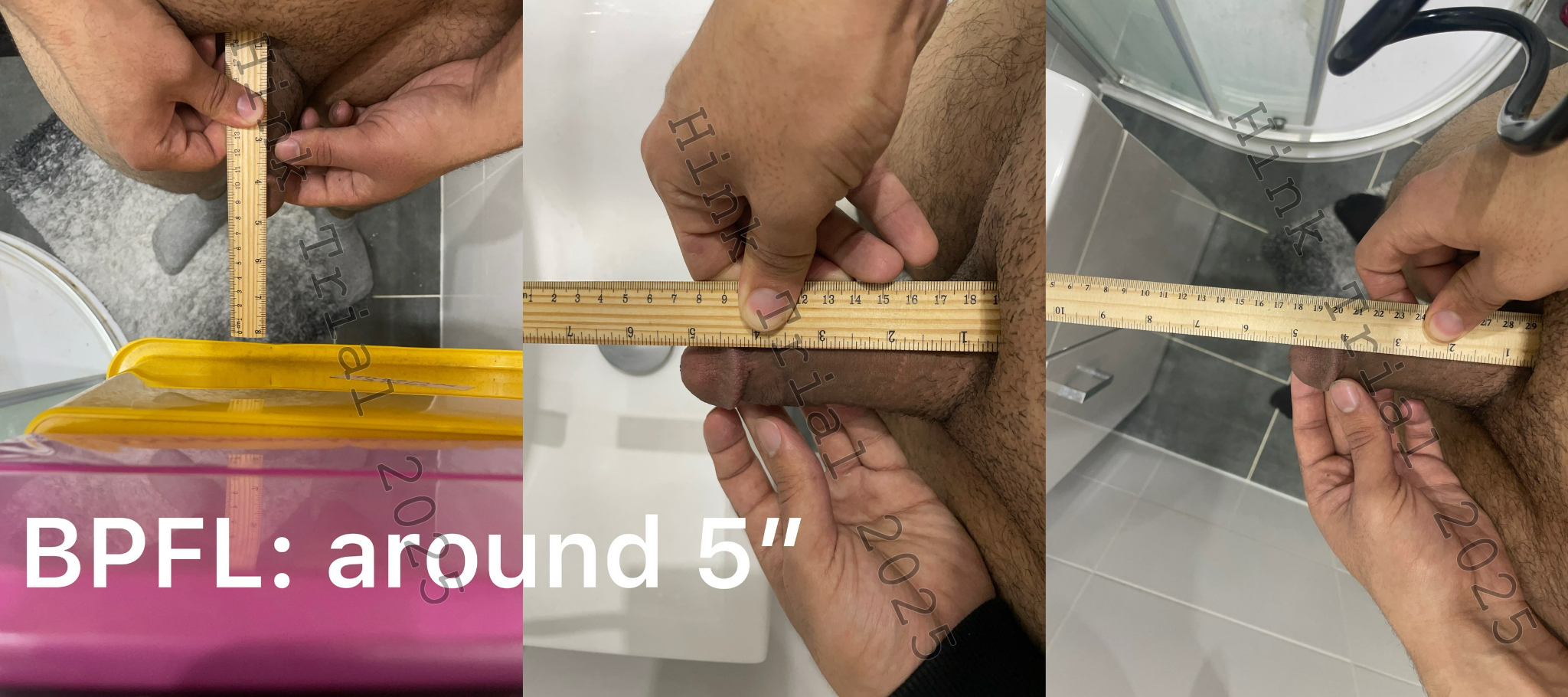
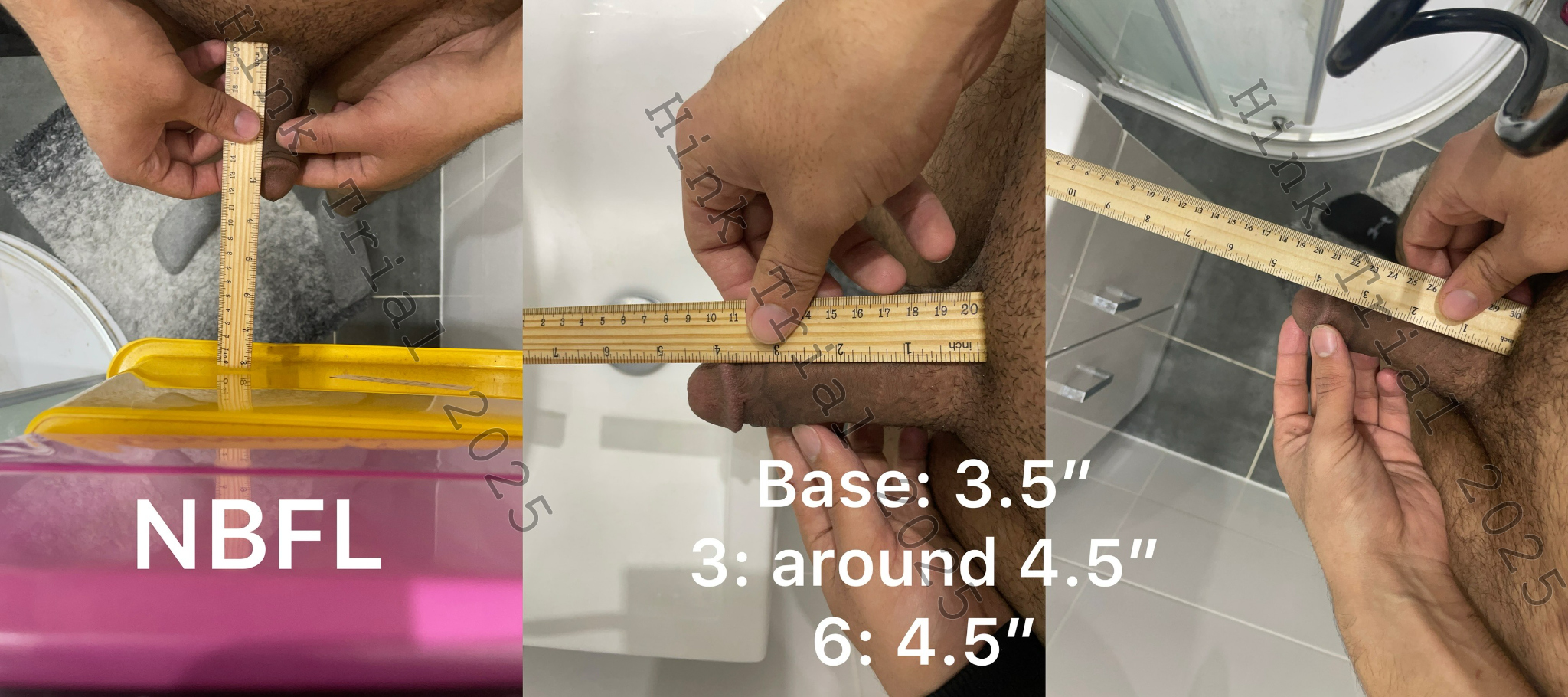
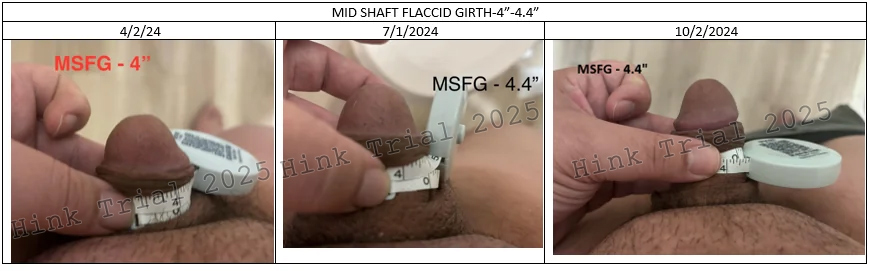
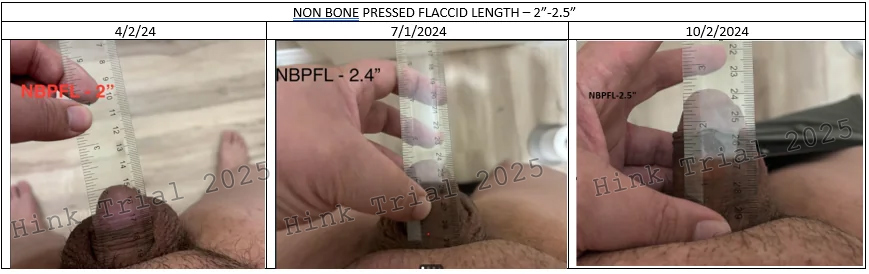
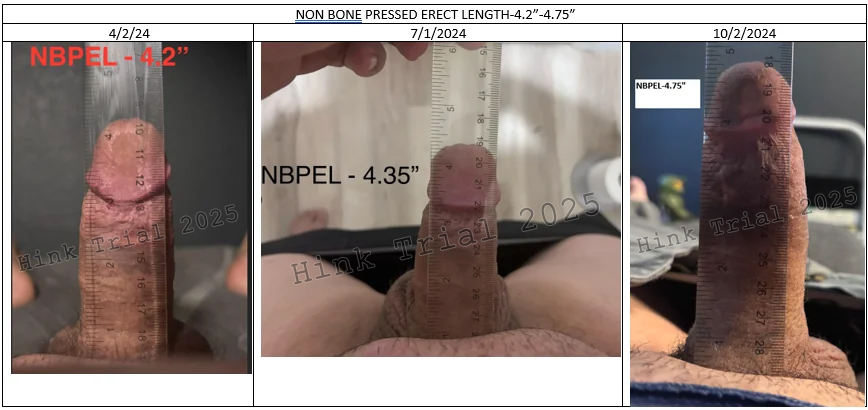
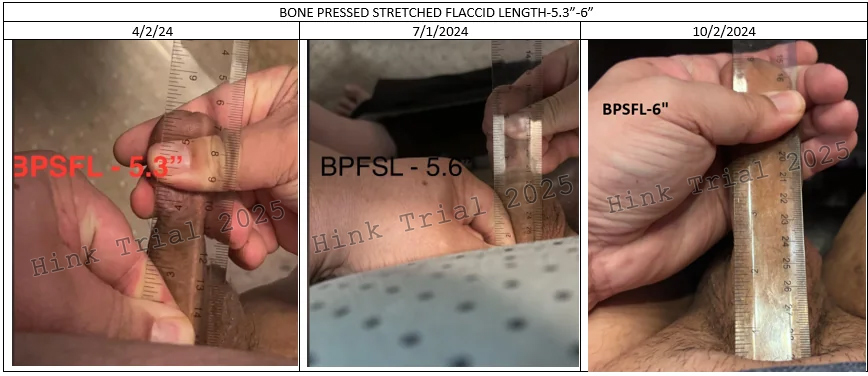
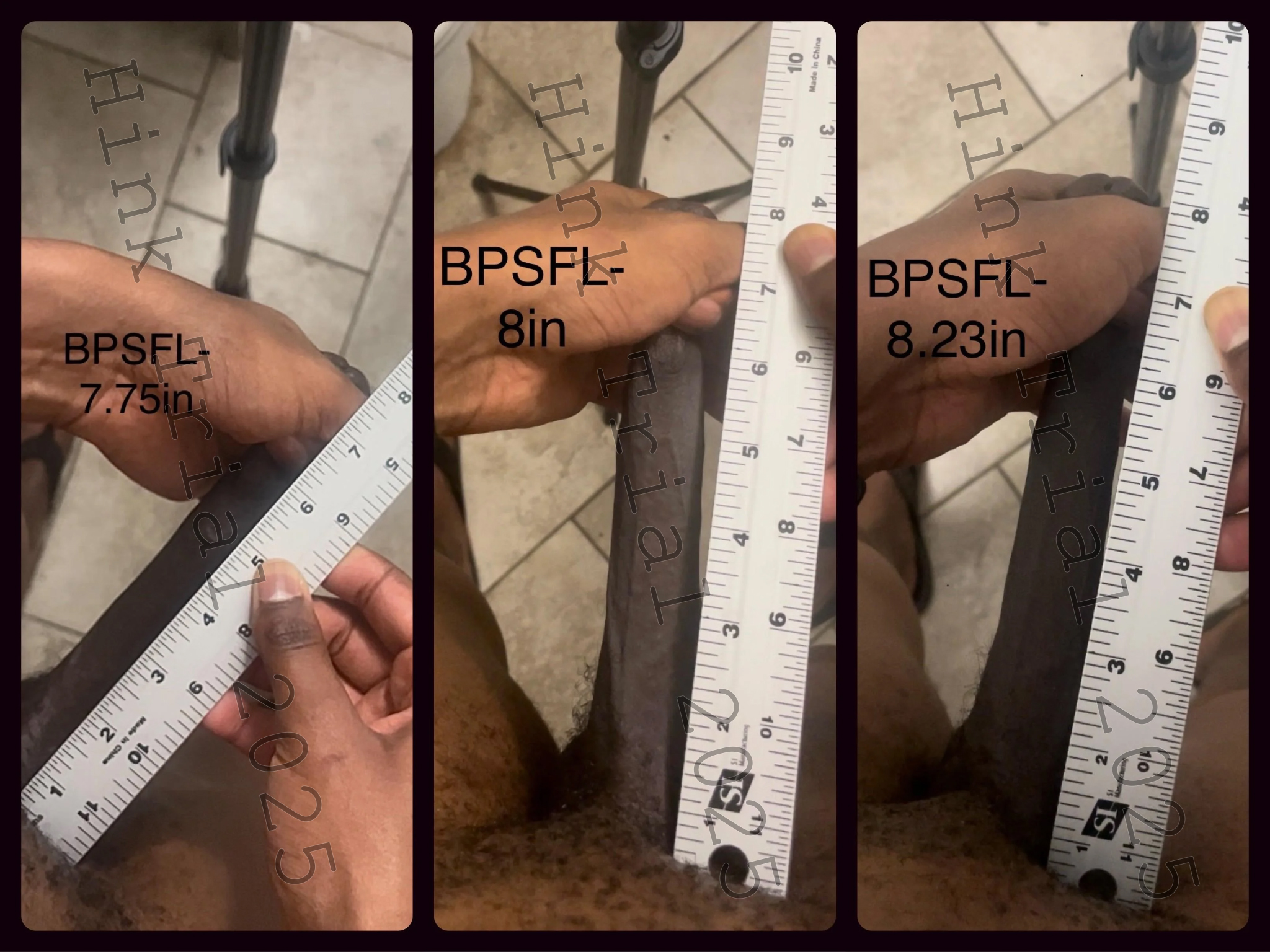
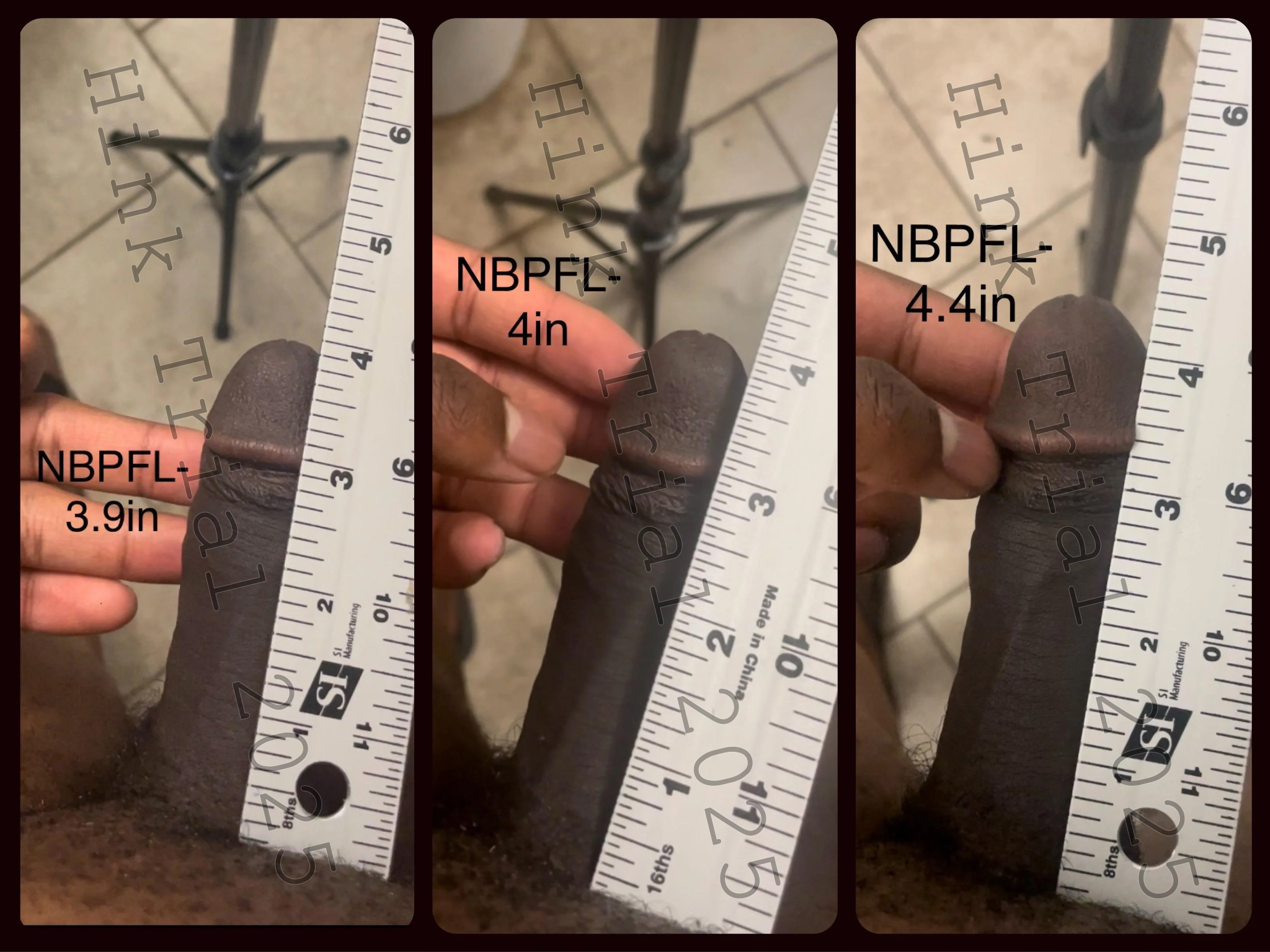
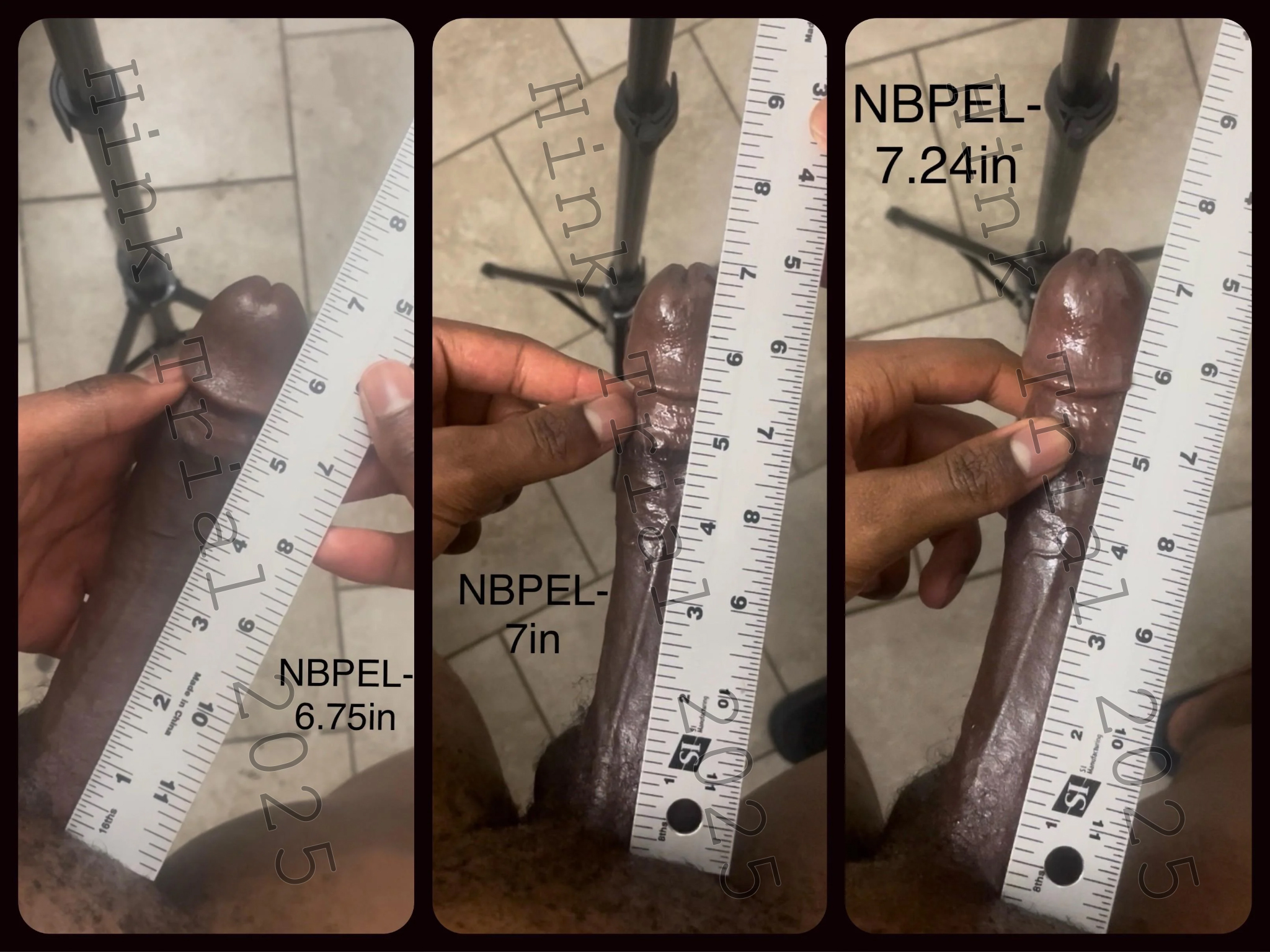
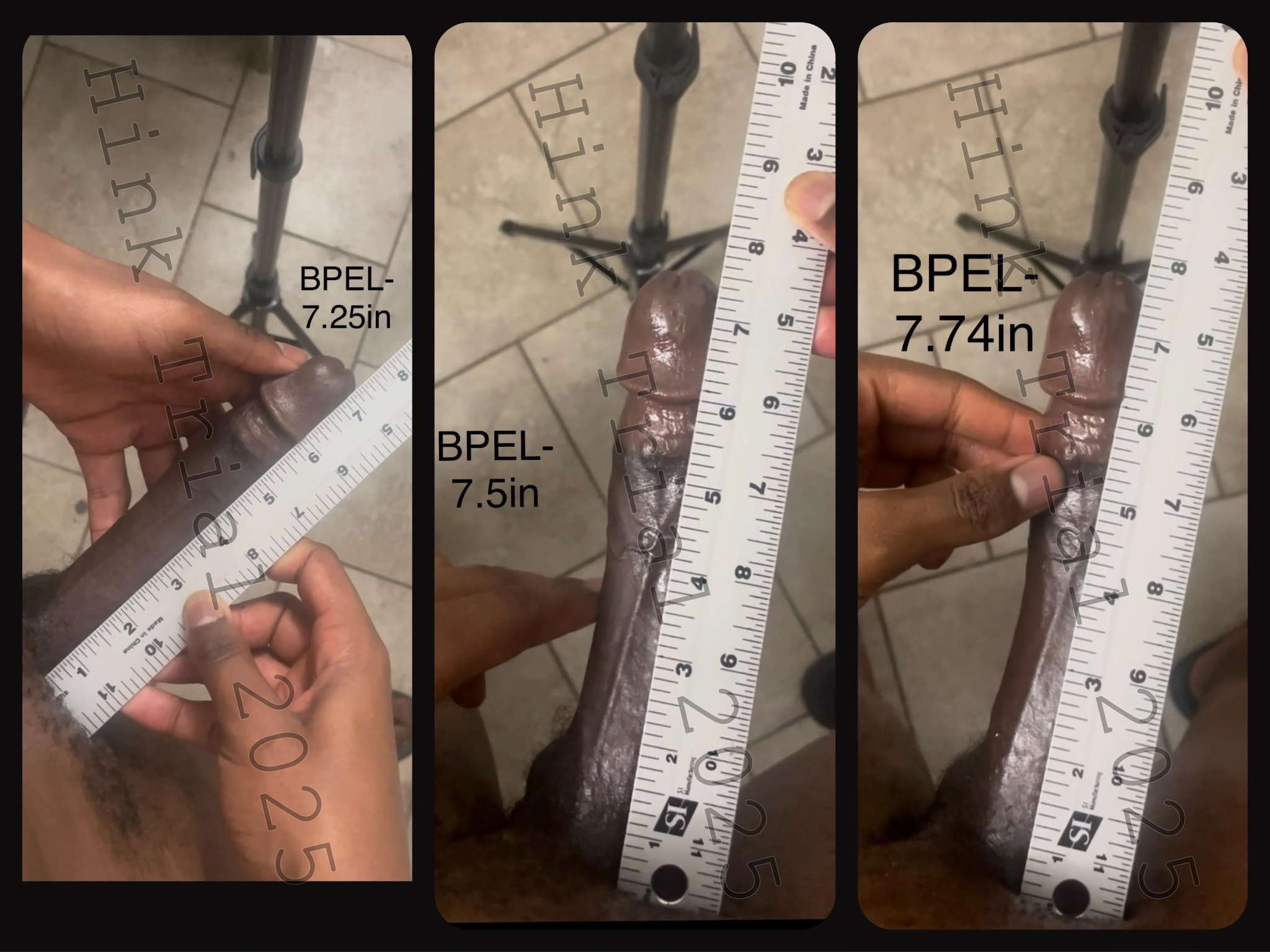
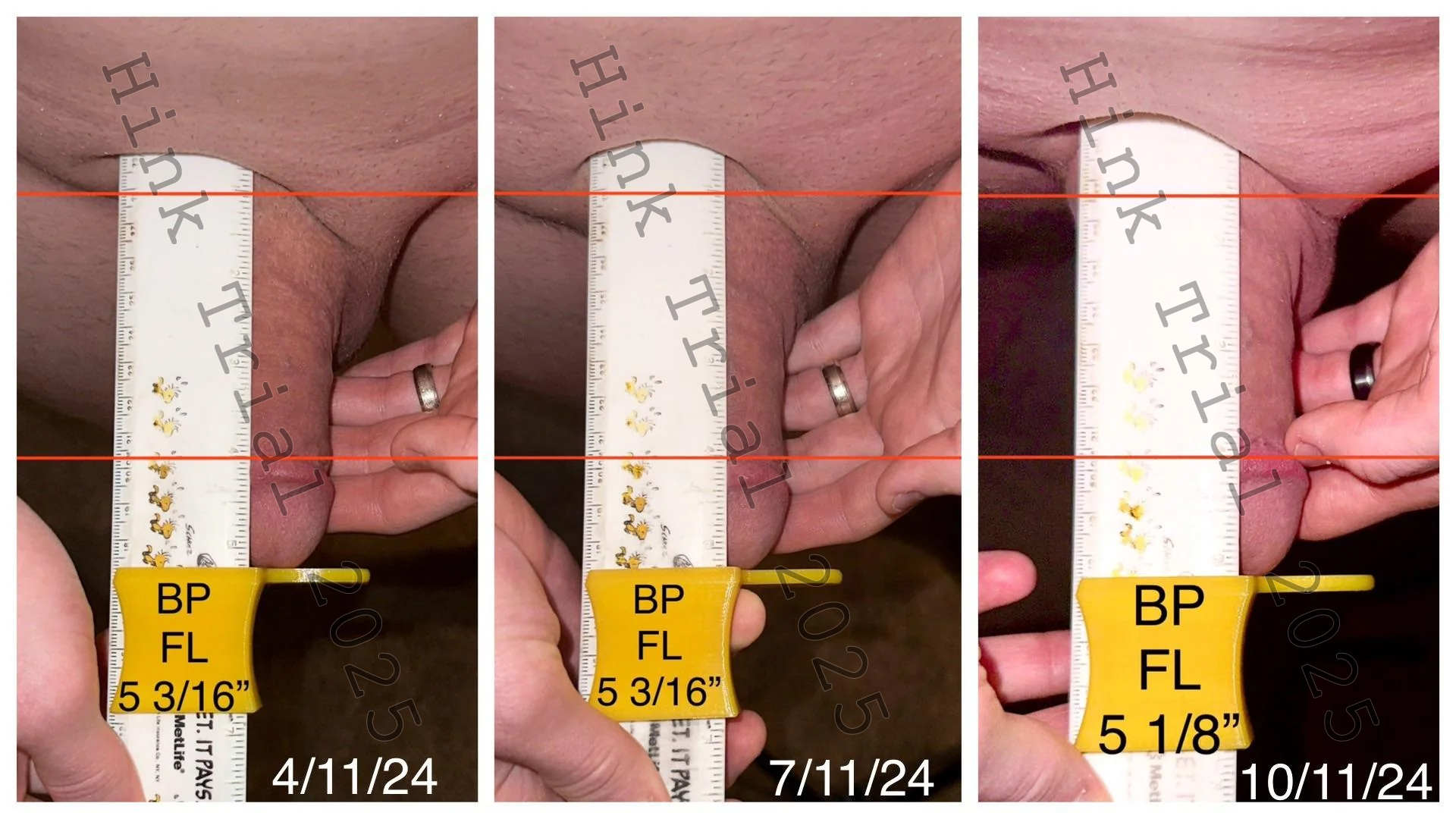
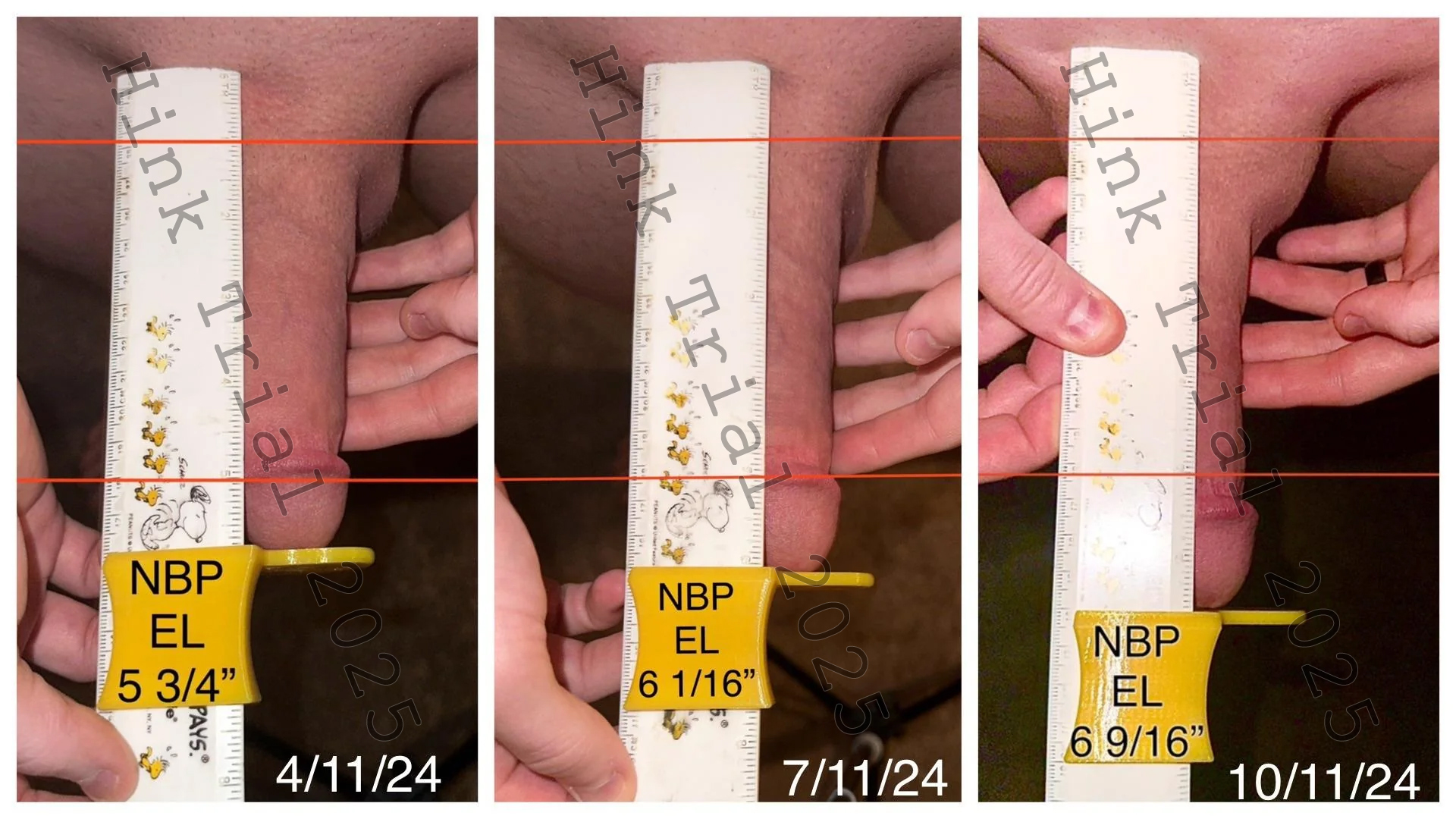
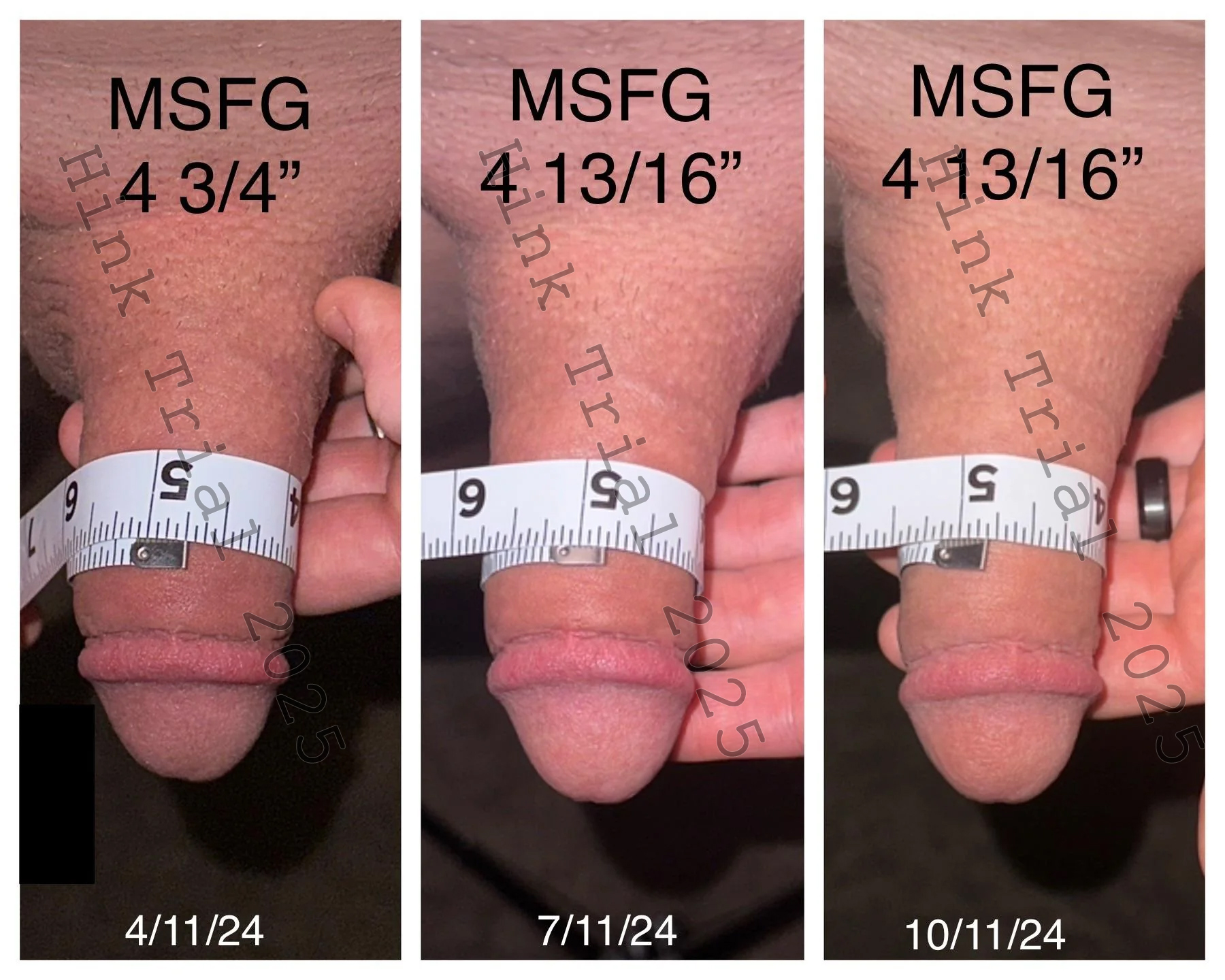
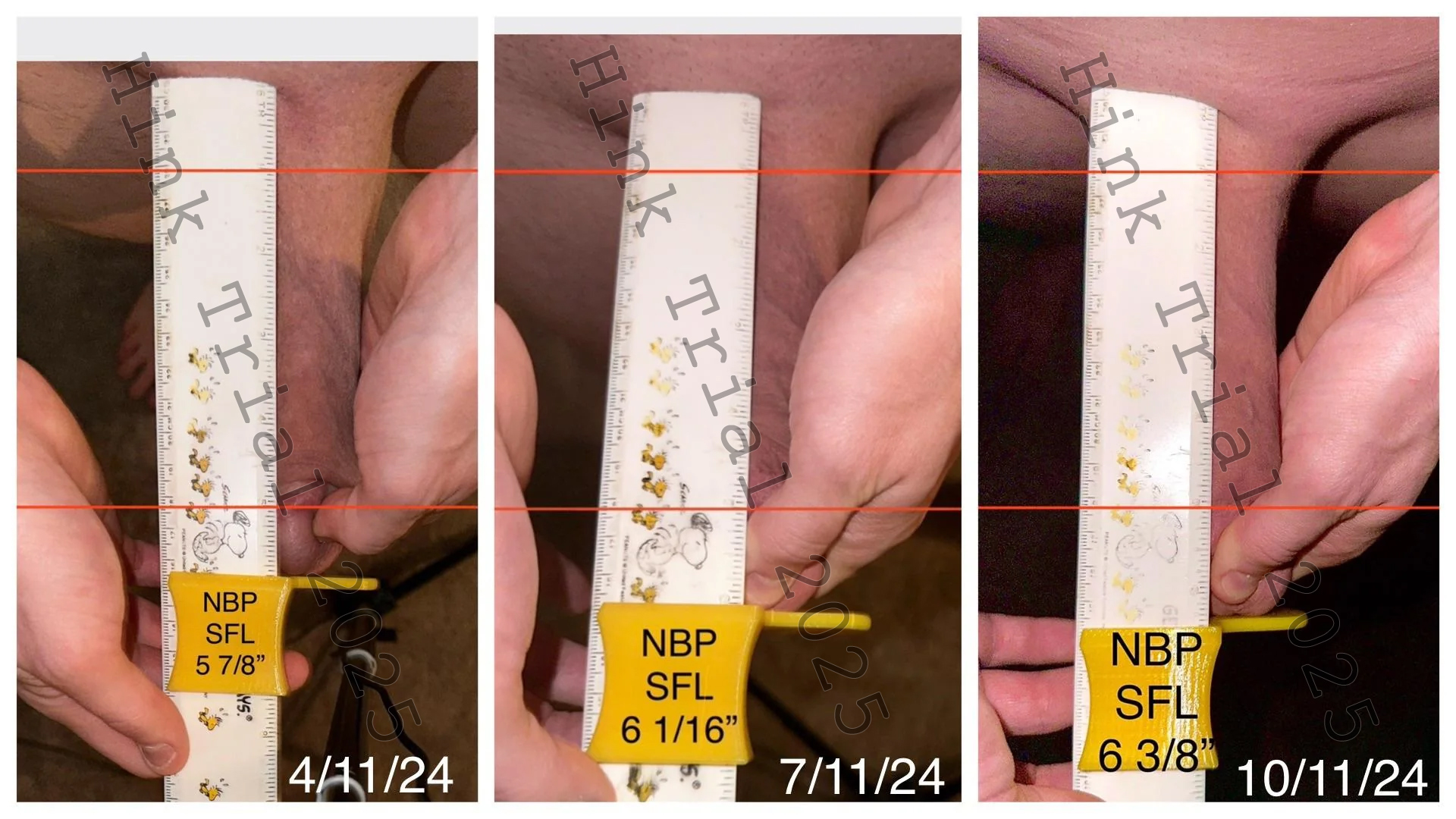
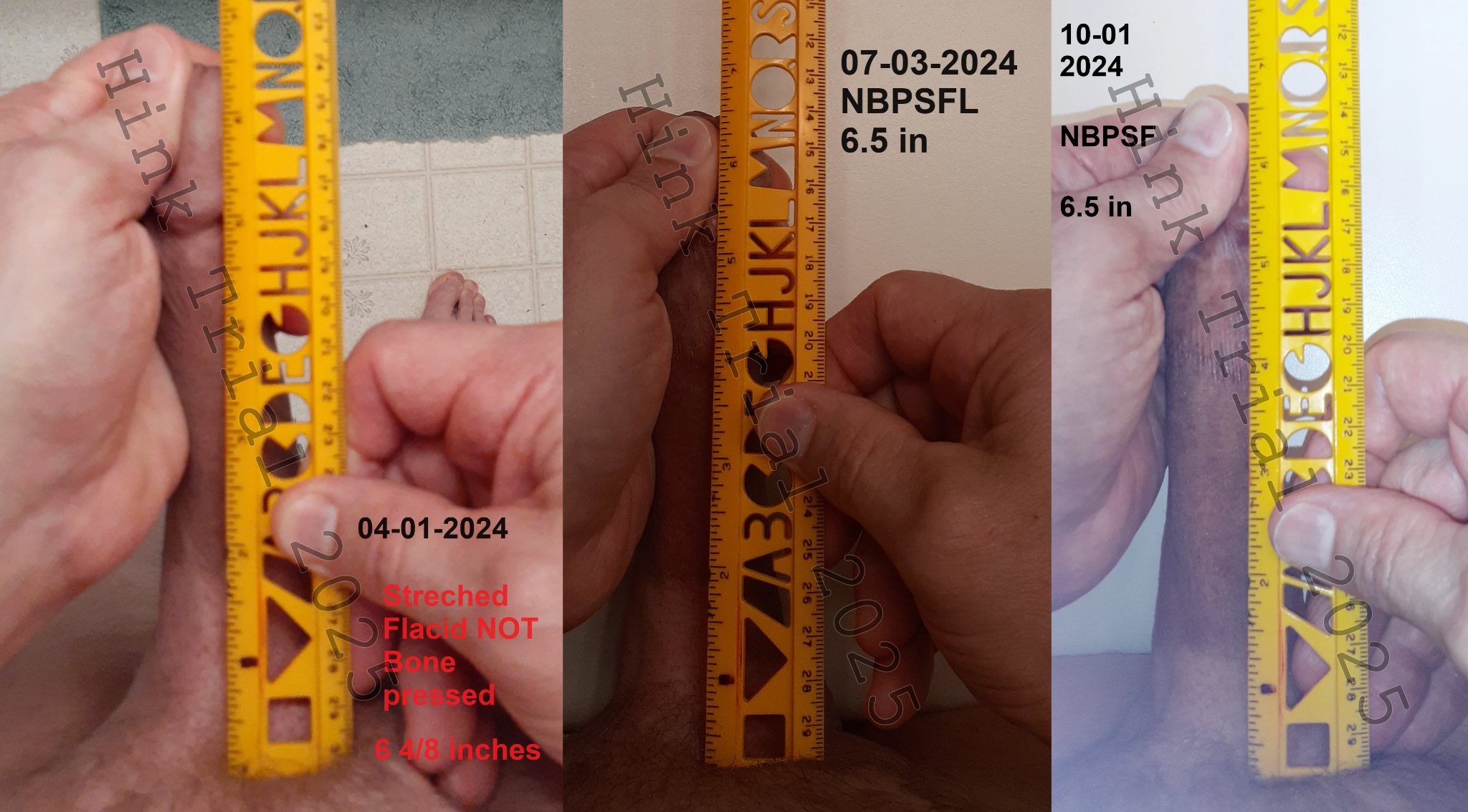
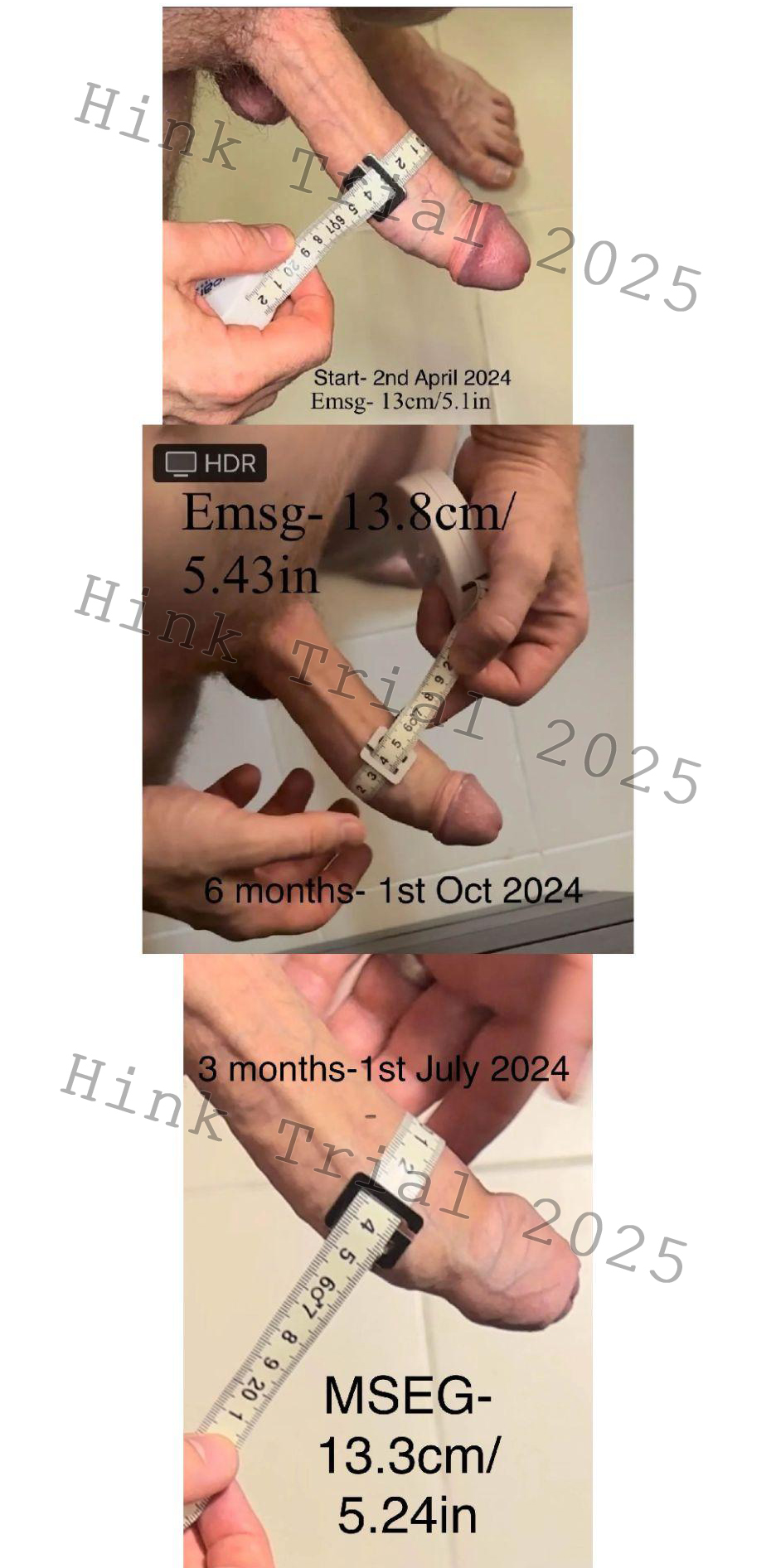
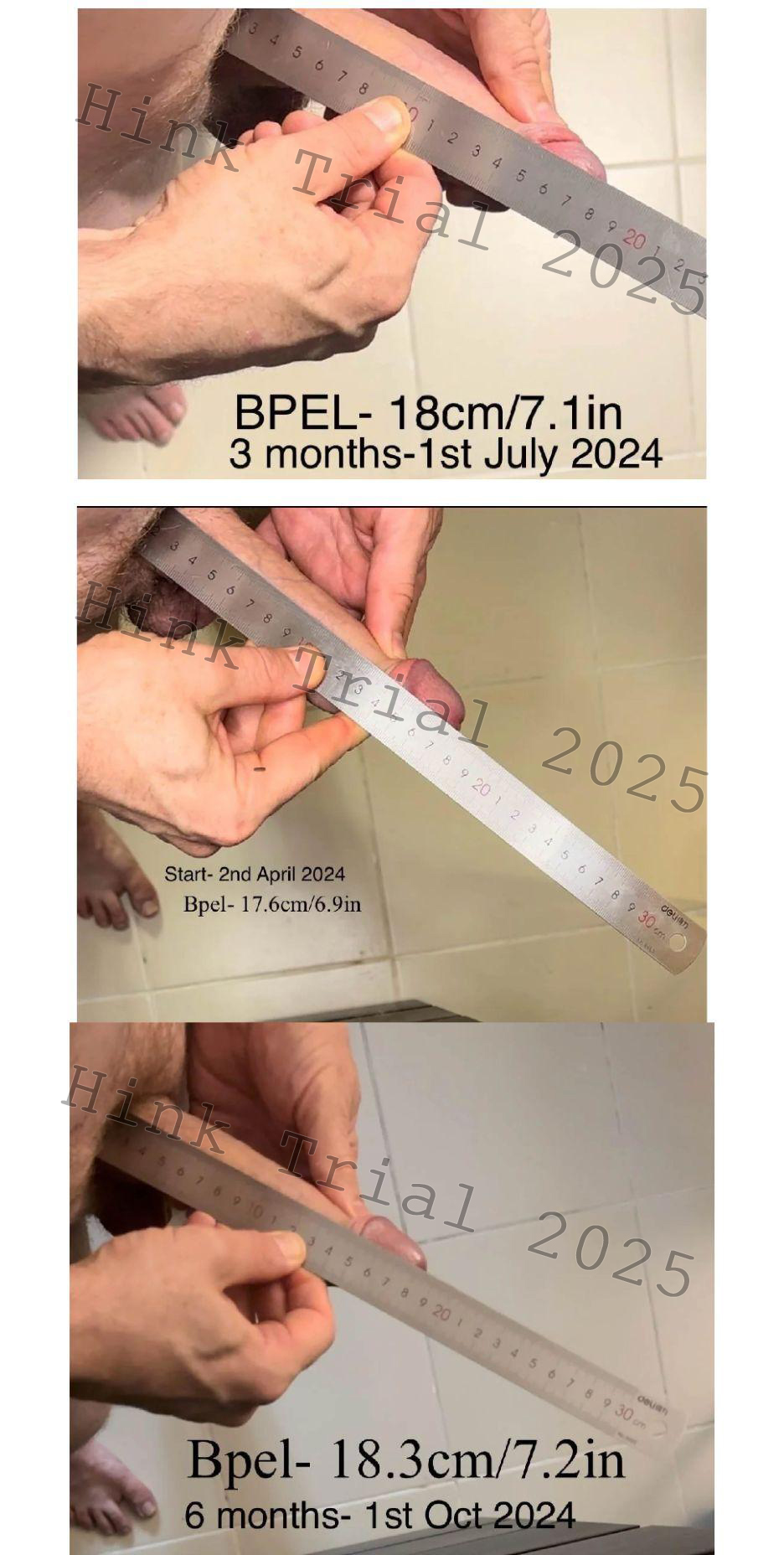
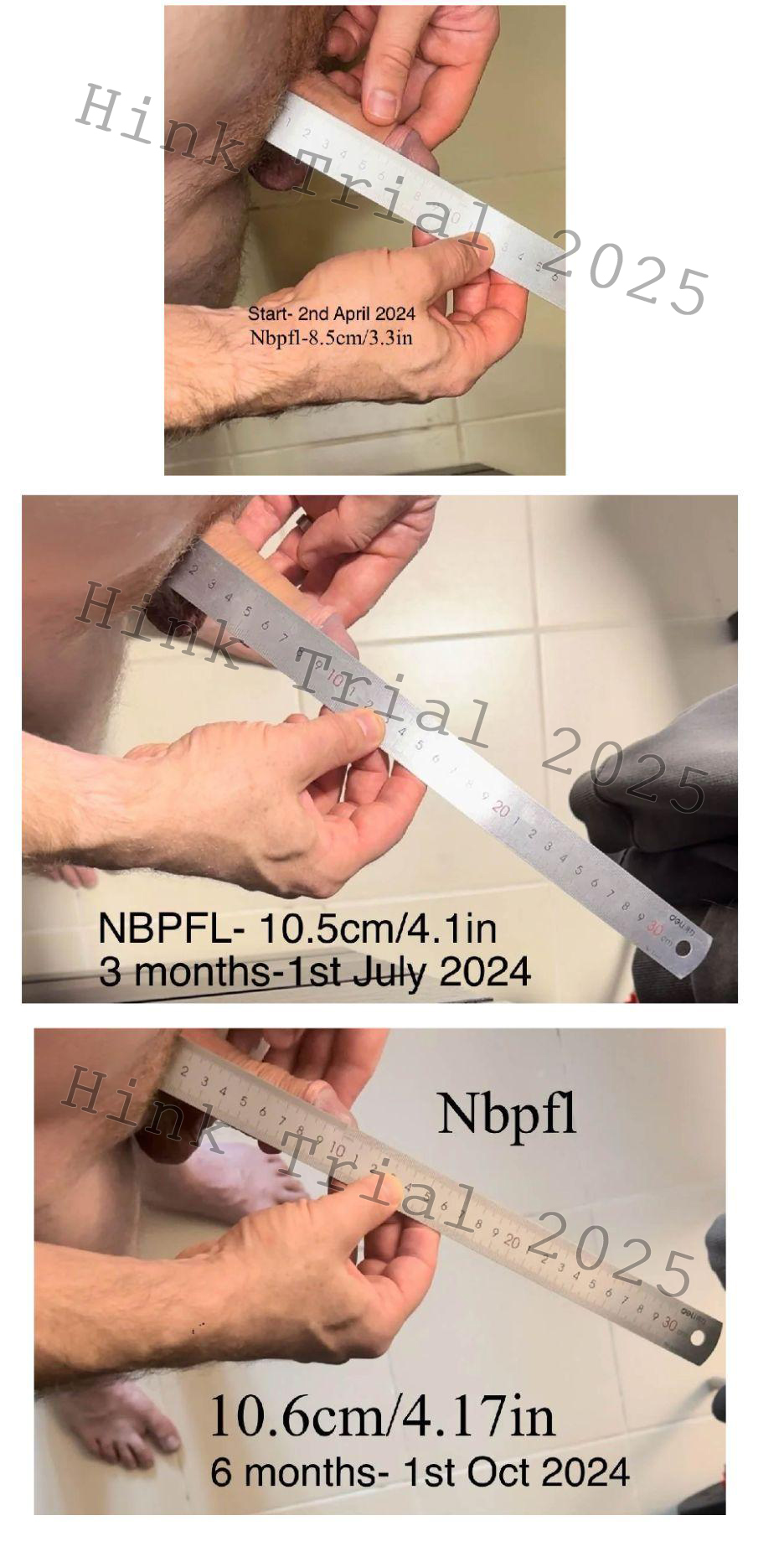
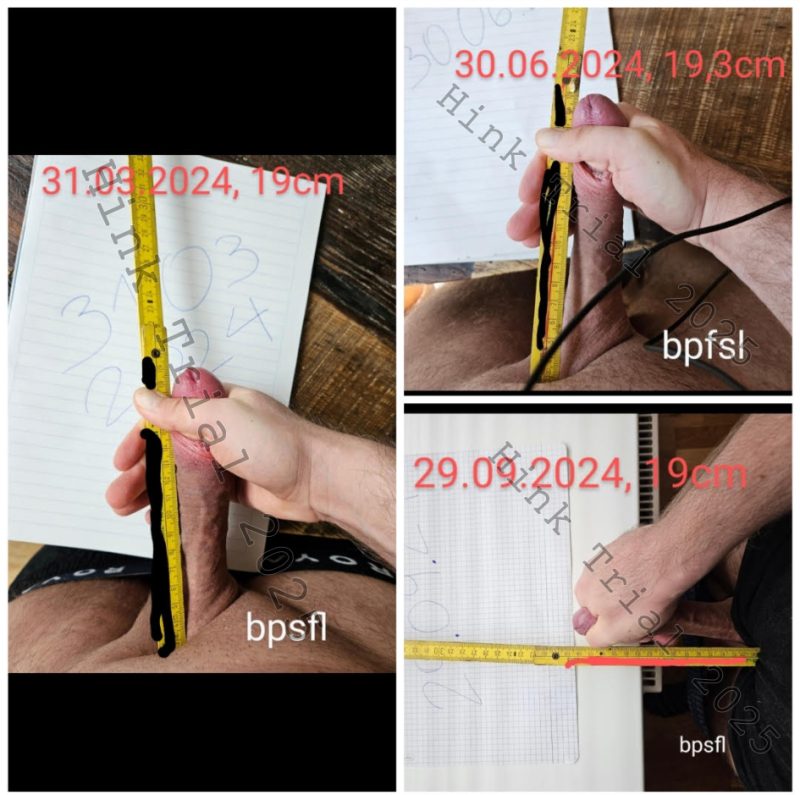
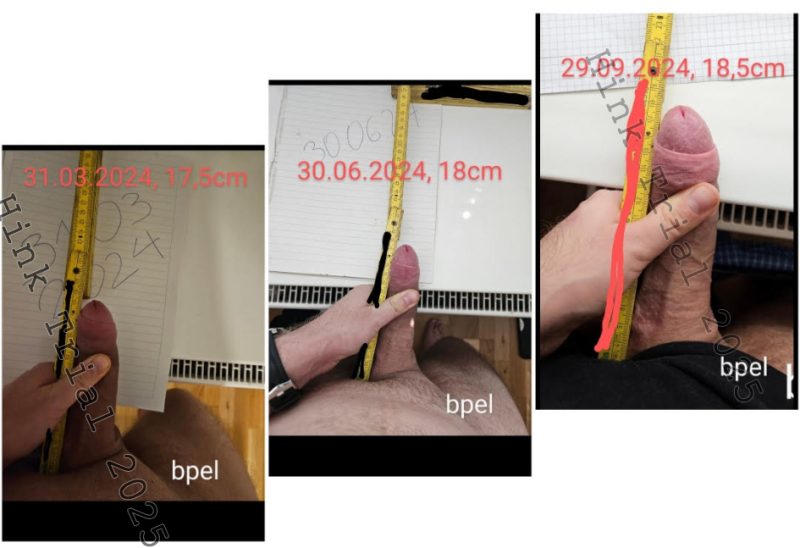
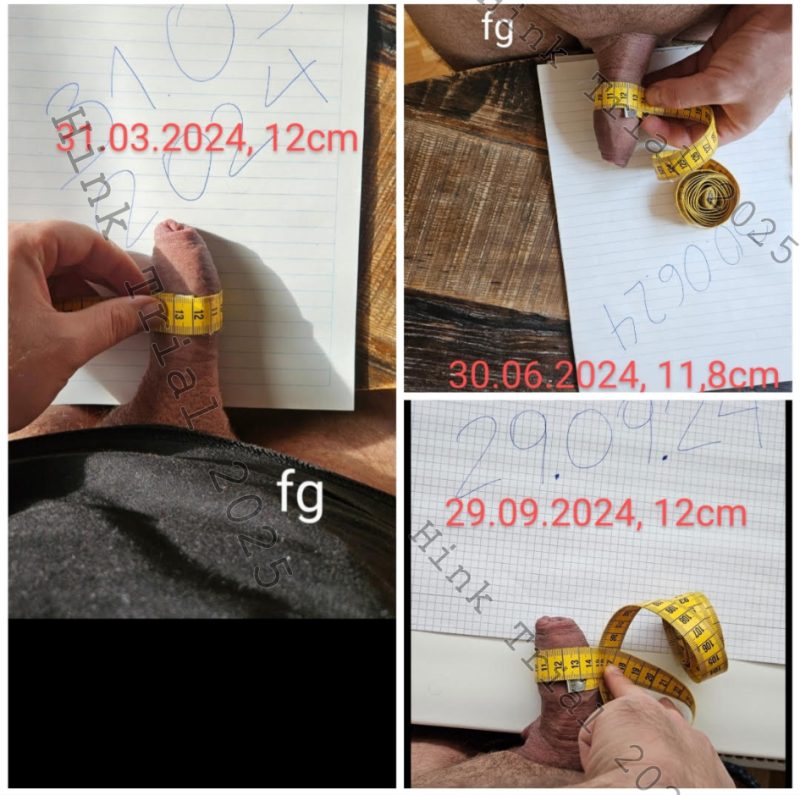
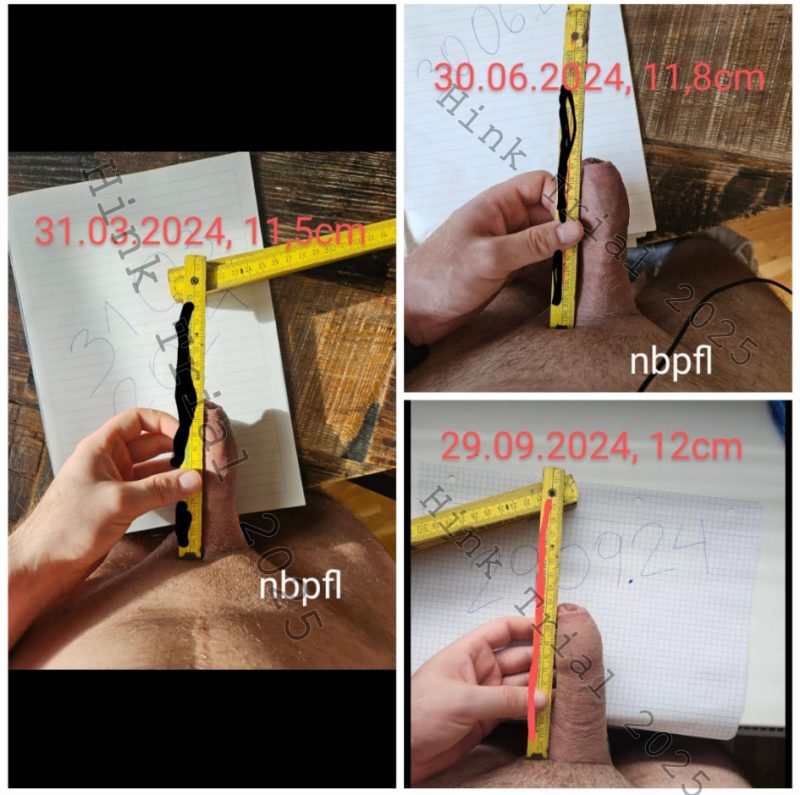
All participants provided written informed consent to document and share the entirety of their enlargement process, including the reporting of adverse events and the submission of standardized pre- and post-intervention photographic evidence. Prior to study initiation, participants were trained in standardized measurement protocols, encompassing bone-pressed erect length (BPEL), non-bone-pressed erect length (NBPEL), mid-shaft erect girth (MSEG), bone-pressed flaccid length (BPFL), and flaccid mid-shaft girth (FG). Measurements were systematically collected at baseline, three months, and six months. To control for potential measurement artifacts related to transient post-exercise edema, all measurements were required to be performed no sooner than two hours following any enlargement exercises.
The enlargement routine for both length and girth was based on Hink’s Enlargement Course (available at Hink’s Site), which details injury prevention strategies and stepwise protocols for penile length and girth training. Participants were advised to take the citrulline-based supplement Vigor (LeviathanSupps.com) at a dosage of ½ to 1 scoop (7–14 grams) approximately 20 to 30 minutes prior to training.
Length training consisted primarily of manual stretching, performed 1–2 times daily for 20–60 minutes, with optional use of penile extenders. A minimum of 30 minutes of manual stretching per day was recommended. Length exercises were to precede girth work in every session.
Girth training was conducted exclusively via vacuum erection pumps, with the recommended model supplied through PeakMalePhysique.com’s “Penis Pump Kit”. The protocol included one warm-up set followed by 3–5 working sets under pressures ranging from 6–12 inHg, targeting a total of at least 20 minutes of time under vacuum daily. Girth exercises were required to follow length exercises immediately.
Participants were initially advised to take two rest days per week during the first month to allow tissue stress adaptation to prevent injury. After this period, rest days were taken as needed based on clinical indicators such as reduced erection quality, pain, bruising, or severe discoloration. Adherence to training at least six days per week was strongly encouraged.
Protocol violations were defined as failure to meet minimum exercise requirements, separation of length and girth work by more than 1 hour, improper photographic documentation, or manipulation of measurements.
Results
A total of 33 participants were enrolled after meeting eligibility criteria, which included verified enrollment in Hink’s Enlargement Course, submission of baseline photographic documentation, and consistent participation in weekly check-ins via the subreddit r/hinktrial2 or via email. By study completion, 7 participants met all predefined criteria for inclusion in the final analysis. Ages of participants ranged between 20 and 45 years old.
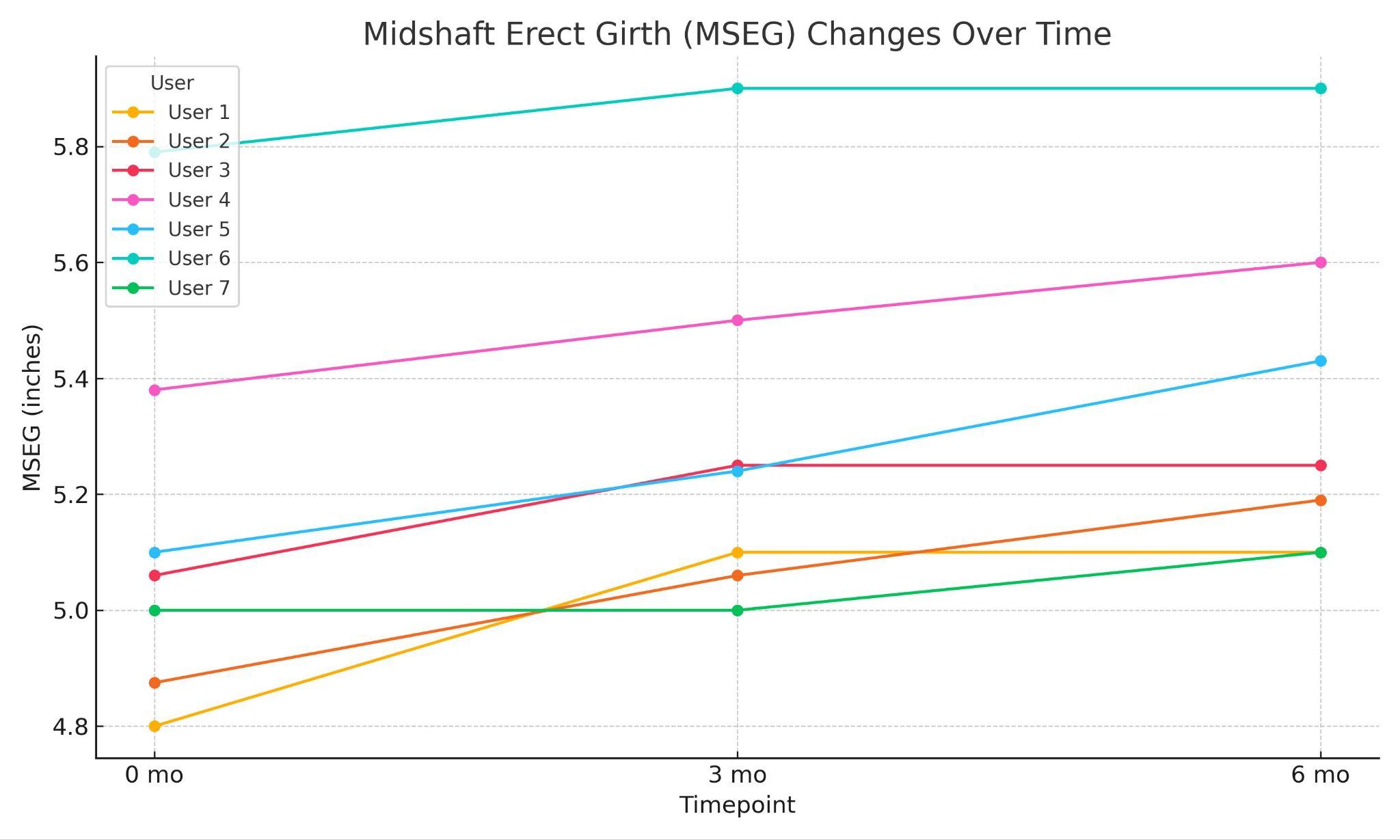
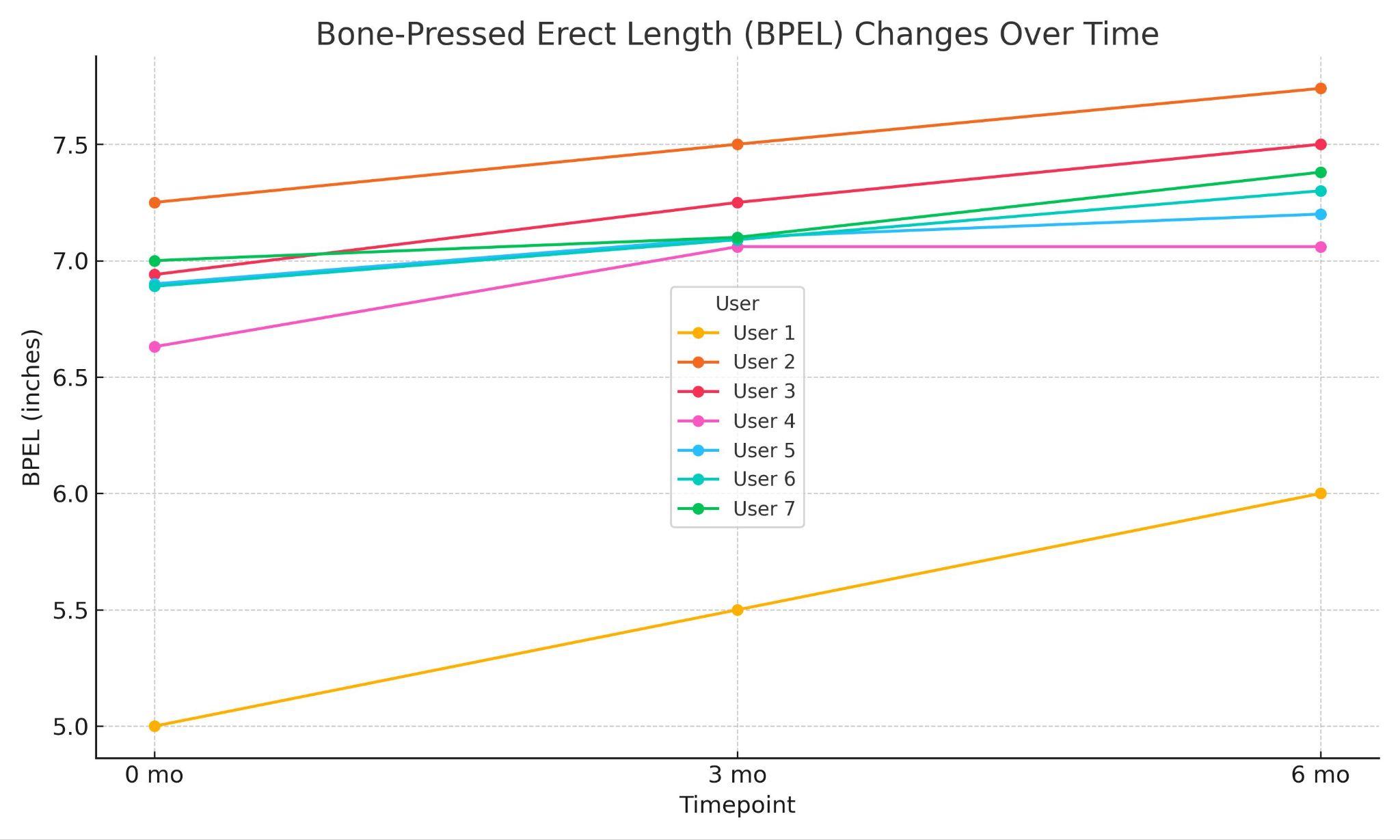
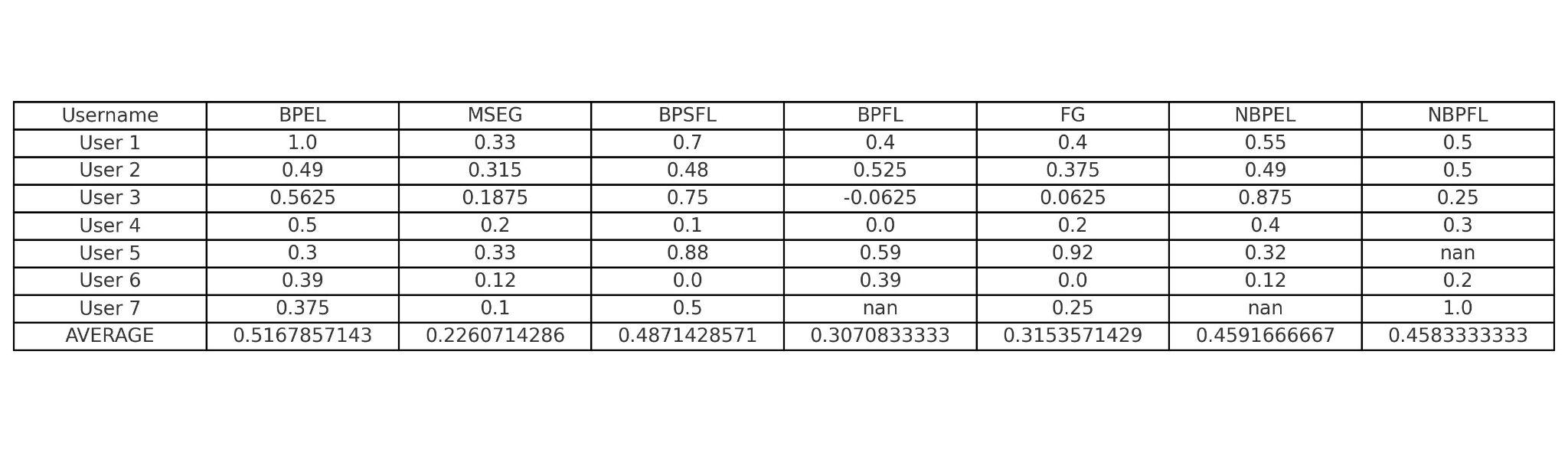
The average baseline bone-pressed erect length (BPEL) was 6.6 inches (16.76 cm), and the average mid-shaft erect girth (MSEG) was 5.14 inches (13.06 cm). Following the intervention, statistically significant increases were observed across multiple penile dimensions. The mean BPEL increased by 0.52 inches (1.32 cm), and the mean MSEG increased by 0.23 inches (0.58 cm). Additional gains were recorded in bone-pressed stretched flaccid length (BPSFL) (+0.49 inches, 1.24 cm) and bone-pressed flaccid length (BPFL) (+0.31 inches, 0.79 cm). Non-bone-pressed measurements demonstrated parallel improvements, with both non-bone-pressed erect length (NBPEL) and non-bone-pressed flaccid length (NBPFL) increasing by 0.46 inches (1.17 cm). Mean flaccid girth (FG) also increased by 0.30 inches (0.76 cm).

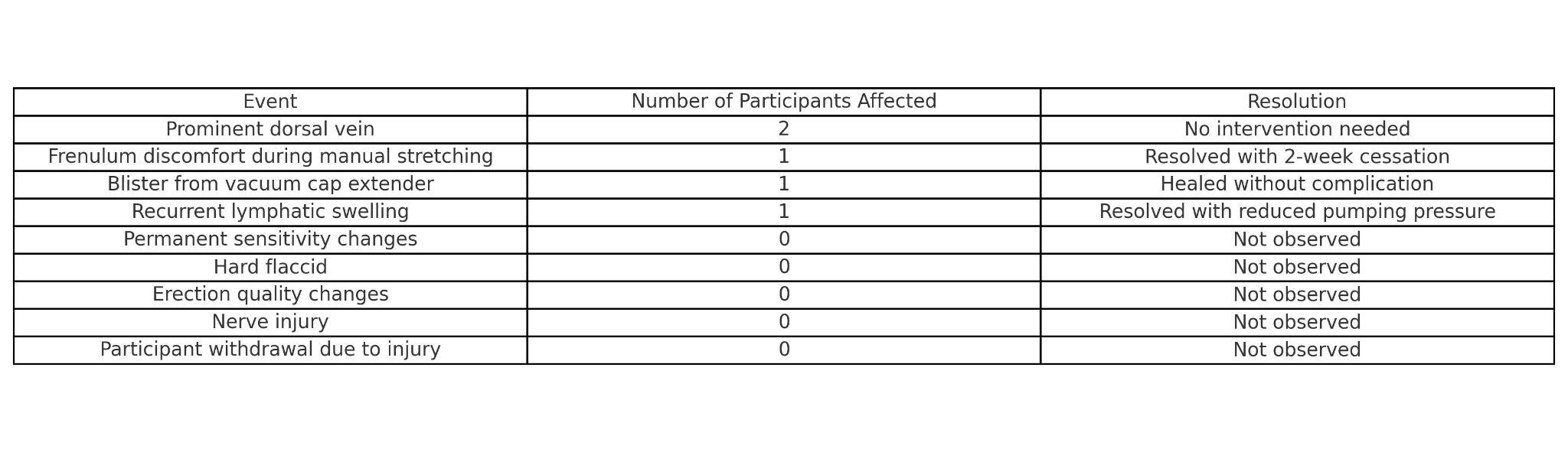
No significant adverse events were observed during the trial period. Two participants noted the development of a more prominent dorsal vein, which was not associated with pain, dysfunction, or adverse clinical outcomes. One participant reported mild discomfort localized to the frenulum during manual stretching exercises; symptoms resolved fully following a two-week interruption in activity, after which the participant successfully resumed the intervention protocol without recurrence. Another participant developed a superficial blister secondary to the use of a vacuum cap extender attachment; the lesion healed without complication, and the participant continued with the assigned regimen. One participant experienced recurrent lymphatic swelling beginning in the fourth month of trial participation; the symptoms resolved spontaneously following a reduction in negative pressure during pumping sessions. Importantly, no participants exhibited any permanent structural or functional penile changes, including alterations in tactile sensitivity, the development of hard flaccid, deterioration in erection quality, or signs of neurovascular injury. Furthermore, no participants withdrew from the study due to penile injury or adverse effects.
Discussion
Non-surgical penile enlargement has long been a subject of controversy, with significant skepticism, including among medical professionals, regarding its efficacy. However, emerging evidence has begun to substantiate its potential. Several studies, including those by Nowroozi et al., have demonstrated that traction-based and negative pressure devices, such as penile extenders and vacuum pumps, can result in measurable increases in penile length. Brandeis et al. further reported gains in both length and girth, although these outcomes were achieved in conjunction with invasive interventions, specifically platelet-rich plasma (PRP) injections. Collectively, these findings support the feasibility of penile enlargement, although mechanisms and results vary depending on the modality.
The Hink Trial is the first prospective study to demonstrate that non-invasive penile enlargement is achievable in both length and girth, with results verified by standardized photographic documentation. Unlike prior studies that lacked objective visual verification and were subject to potential bias, this trial incorporated verified imaging to allow for transparent and reproducible assessment of outcomes. Importantly, the intervention excluded all surgical procedures and injectable therapies. It is also the first study to document measurable girth enhancement using a vacuum erection device, setting it apart from earlier research that focused predominantly on length.
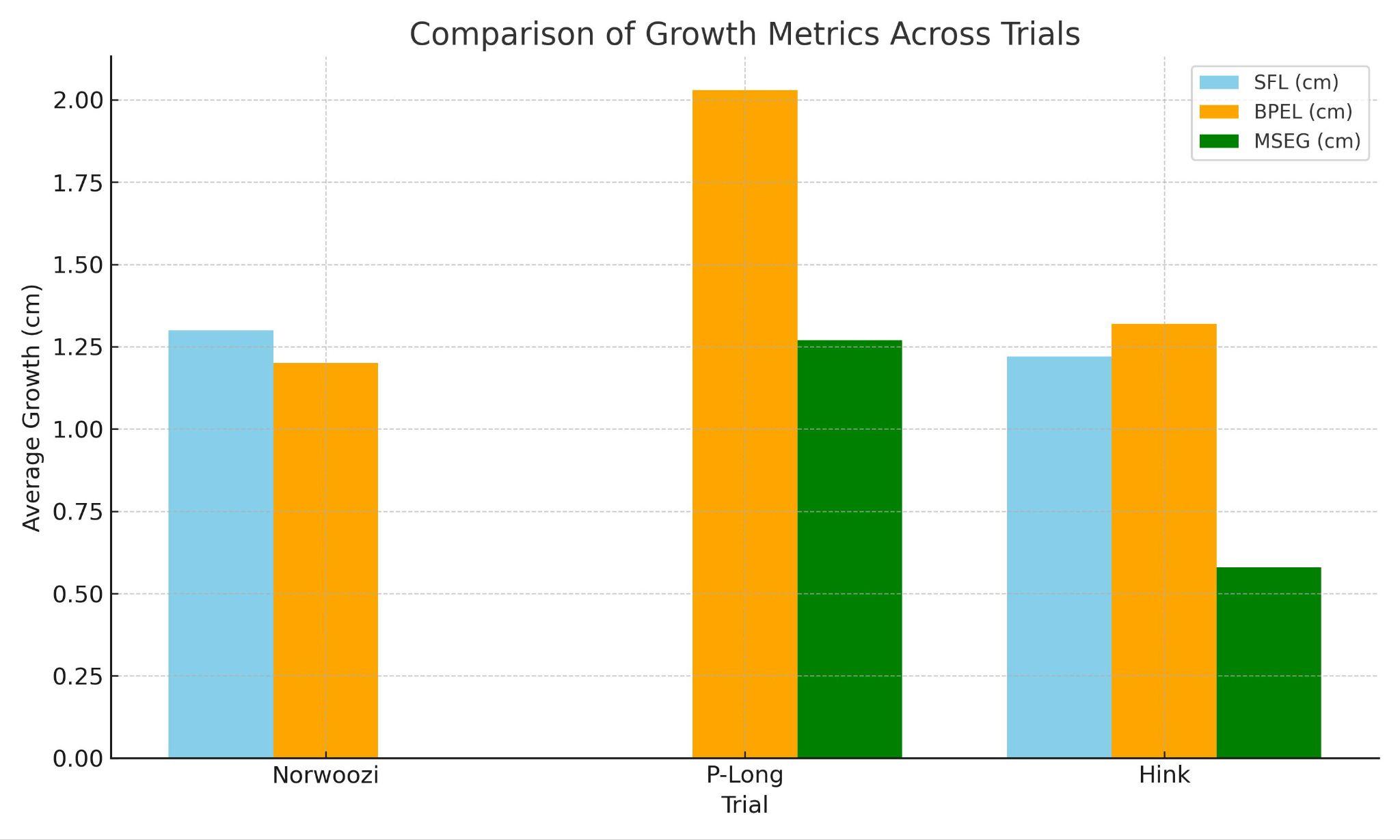
When comparing outcomes among the Norwoozi, P-Long, and Hink trials, all demonstrated measurable improvements in penile dimensions, although their methodologies differed substantially. The Norwoozi trial reported mean increases of 1.3 cm (0.51 inches) in stretched flaccid length (SFL) and 1.2 cm (0.47 inches) in bone-pressed erect length (BPEL), but did not report girth measurements, limiting its comprehensive applicability. The P-Long trial, which combined traction, vacuum therapy, and PRP injections, demonstrated greater overall gains, with mean increases of 2.03 cm (0.8 inches) in BPEL and 1.27 cm (0.5 inches) in mid-shaft erect girth (MSEG). However, no photographic evidence was provided to validate these results.
In contrast, the Hink Trial demonstrated comparable improvements, with mean gains of 1.22 cm (0.48 inches) in SFL, 1.32 cm (0.52 inches) in BPEL, and 0.58 cm (0.23 inches) in MSEG, achieved exclusively through non-invasive methods and documented with photographic evidence. Although the P-Long study reported larger mean changes, its reliance on invasive therapies and the absence of visual verification highlight the advantages of the accessible and transparent methodology employed in the Hink Trial.
These findings exceed the author’s previous observational data, which suggested conservative annual growth rates of approximately 0.5 inches (1.27 cm) in BPEL and 0.25 inches (0.64 cm) in MSEG among individuals engaging in enlargement exercises. This is consistent with the findings of Wikman et al. (2025), where a reported gain rate of 0.1 inches (2.54 mm) per 26 ± 10 hours of training extrapolates to approximately 0.4 inches (1.02 cm) annually, aligning with the minimum exercise volume recommended in the Hink Trial protocol. Notably, the concurrent performance of length and girth exercises appeared to produce gains that exceeded expectations. It is hypothesized that performing these exercises in combination may have a synergistic effect, enhancing both parameters simultaneously. This observation challenges the traditional belief that length and girth training should be performed separately to optimize outcomes.
This study is distinguished by its efficiency. Participants achieved outcomes comparable to prior traction studies, such as those by Nowroozi et al., with an average of approximately 30 minutes of manual stretching and 20 minutes of vacuum pumping per day. This is substantially less than the 3 to 6 hours of daily device use often required by extender-based protocols. The reduced time commitment may enhance adherence and broaden the practical applicability of the intervention.
Growth patterns revealed that approximately half of participants achieved the majority of their girth gains within the first three months, after which a plateau effect was observed. Conversely, BPEL largely continued to increase monthly with no plateau. Increases in SFL closely paralleled gains in BPEL, further supporting the use of SFL as an early predictive measure of penile growth.
No serious injuries were observed, supporting the safety of these non-invasive protocols when performed correctly under appropriate guidance. Although no technique is entirely without risk, these results contribute to the growing body of evidence suggesting that structured programs can be performed safely. The potential endothelial protective effects of the citrulline-based supplement Vigor are acknowledged, although they remain speculative.
Cost efficiency also strengthens the accessibility of the protocol. Participants primarily used the zero cost manual techniques from Hink’s Enlargement Course and a commercially available pump system costing less than $90. This is markedly lower than the financial burden associated with protocols such as P-Long, which require PRP injections and specialized equipment.
Future research should focus on conducting large, prospective cohort studies under urologic supervision to further establish the efficacy, safety, and legitimacy of non-surgical penile enlargement strategies.
Limitations
This study has several limitations. First, the final sample size was small, with only 7 of the original 33 participants completing the protocol according to predefined criteria. This high attrition rate limits the generalizability of the findings, although similar patterns of attrition have been observed in previous penile enlargement studies. Aside from a few participants who failed to meet eligibility requirements due to protocol violations, most discontinued participants either deleted their usernames or ceased responding to follow-up communications.
Second, although photographic documentation was required, variability in image reproducibility introduced challenges for consistent and objective evaluation. Third, some heterogeneity in the intervention protocol was observed; a minority of participants incorporated adjunctive methods such as traction devices (extenders) or intermittent soft clamping in addition to the prescribed manual stretching and pumping regimen, potentially introducing confounding variables.
Additionally, baseline penile dimensions among participants were notably above average, suggesting possible selection bias and limiting the applicability of the findings to the broader population. Lastly, while measurable trends in penile growth were documented, the small cohort size restricted the ability to conduct robust inferential statistical analyses beyond descriptive reporting. Future studies would benefit from extended follow-up periods after cessation of enlargement exercises to confirm the durability and permanence of observed gains.
Conclusions
The Hink Trial represents the first prospective cohort study to conclusively demonstrate that both penile length and girth can be increased in the erect and flaccid states using entirely non-surgical, non-invasive techniques. Importantly, it is also the first trial to provide photographic documentation to objectively validate these outcomes. These findings offer a critical foundation for future randomized controlled trials aimed at establishing the highest level of clinical evidence for non-surgical penile enhancement.
Despite its limitations—including a small final sample size and participant variability—this study provides meaningful evidence that safe, consistent application of non-invasive protocols can lead to measurable, clinically relevant improvements. The results may encourage greater adherence to non-surgical approaches and help deter individuals from pursuing riskier surgical interventions in pursuit of penile enlargement goals.
Disclosure
Participants were reimbursed for the cost of Hink’s Enlargement Course and received a $100 honorarium upon completion of the study and submission of data, including consented photographic documentation. The author of this study has direct financial ties to peakmalephysique.com (Pump) and leviathansupps.com (Vigor).
Acknowledgements
I would like to extend my sincere gratitude to Grant from Peak Male Physique for his valuable support and contributions throughout the project. Special thanks are also given to Cali for his assistance in organizing and facilitating the trial. Appreciation is extended to “B” in Costa Rica for managing and maintaining the trial subreddit community, and “WakingDream” for editing and web development.
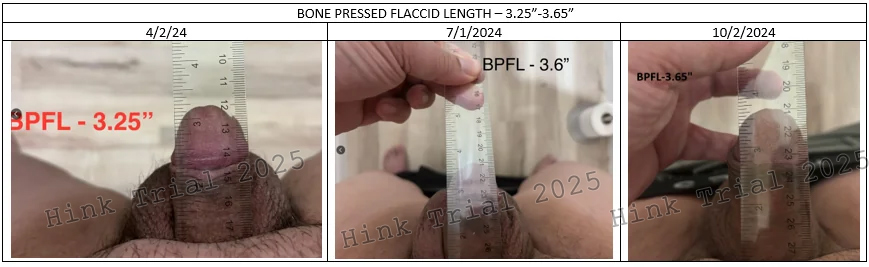
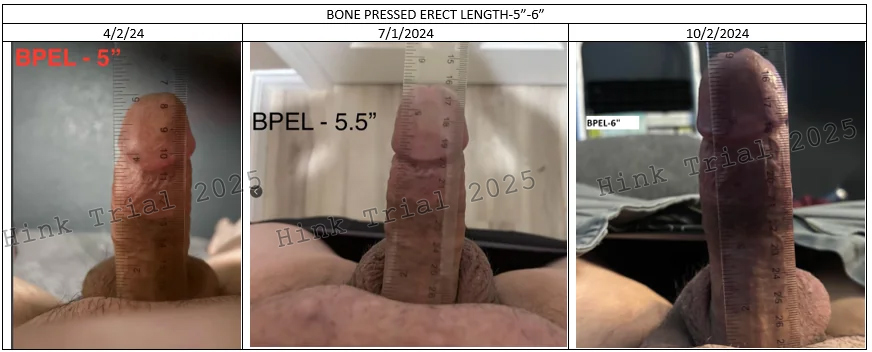
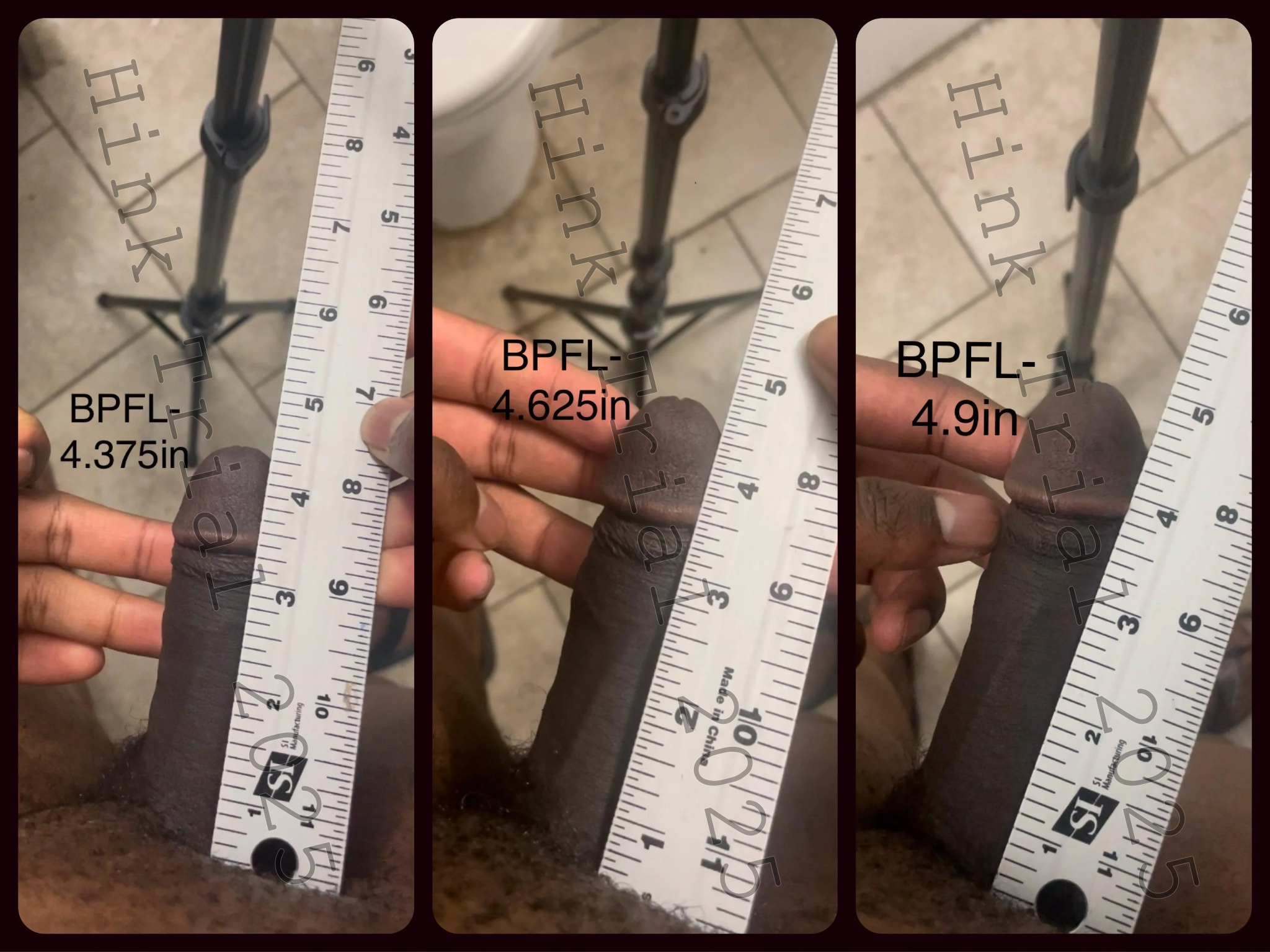
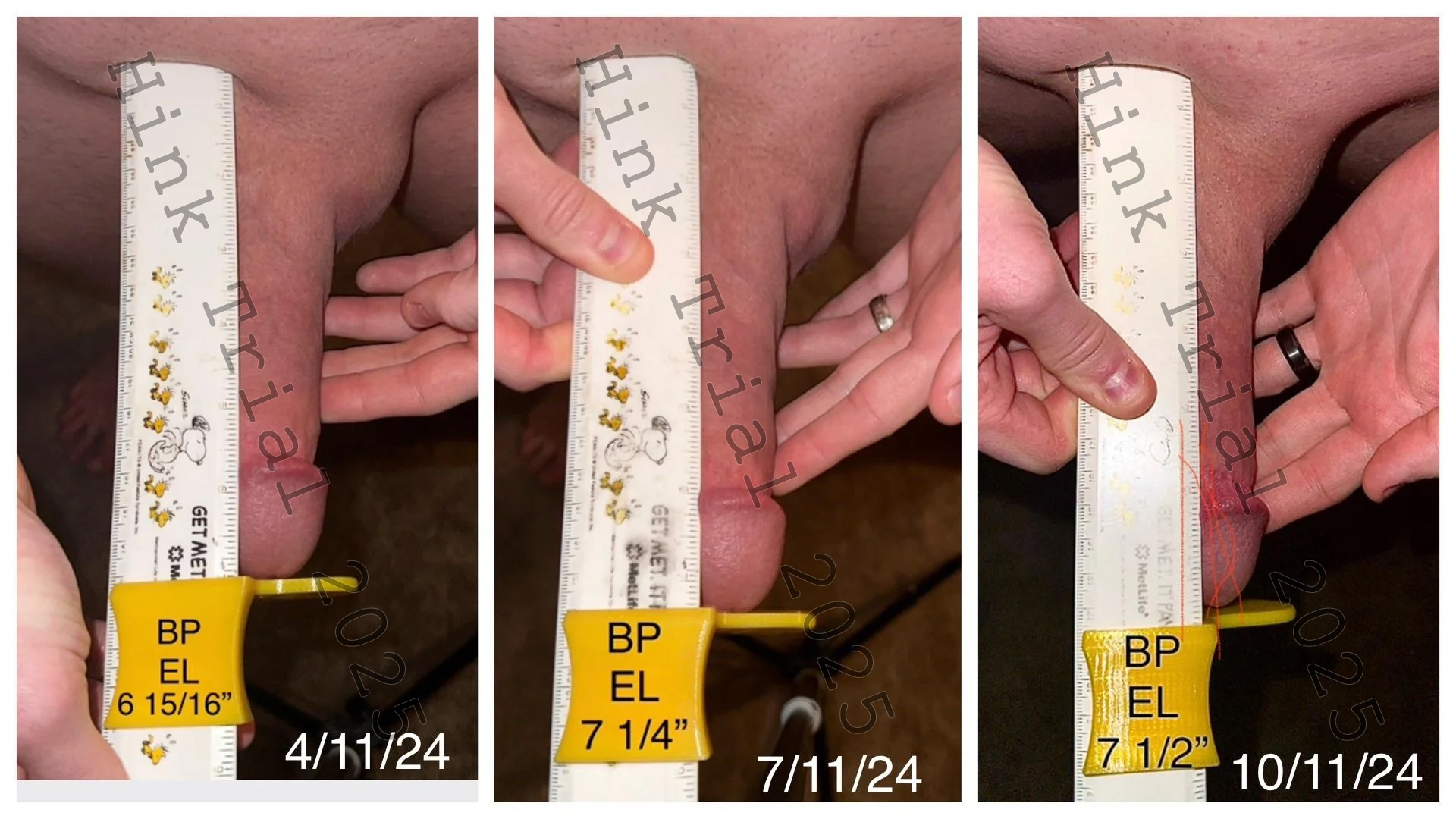
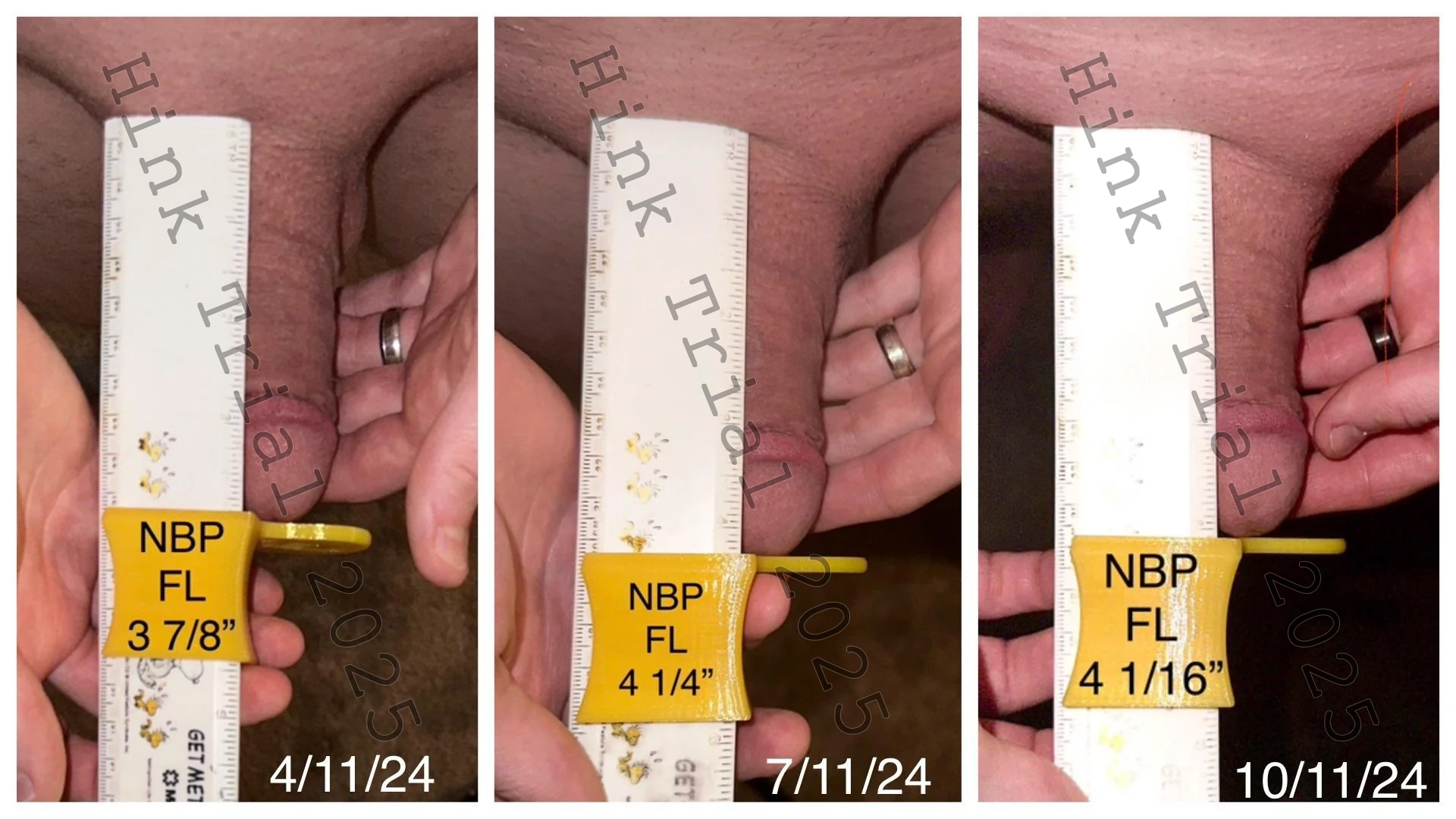
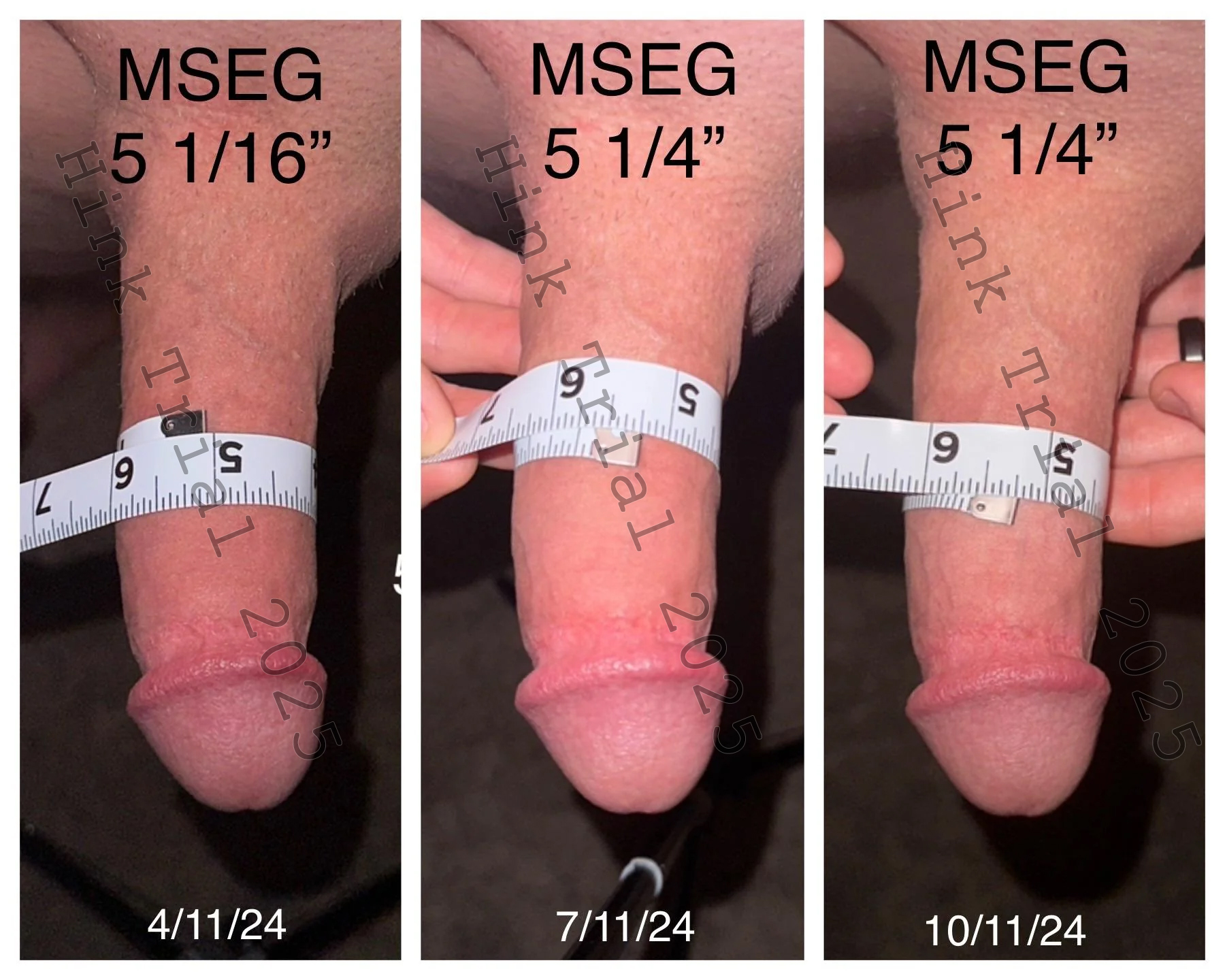
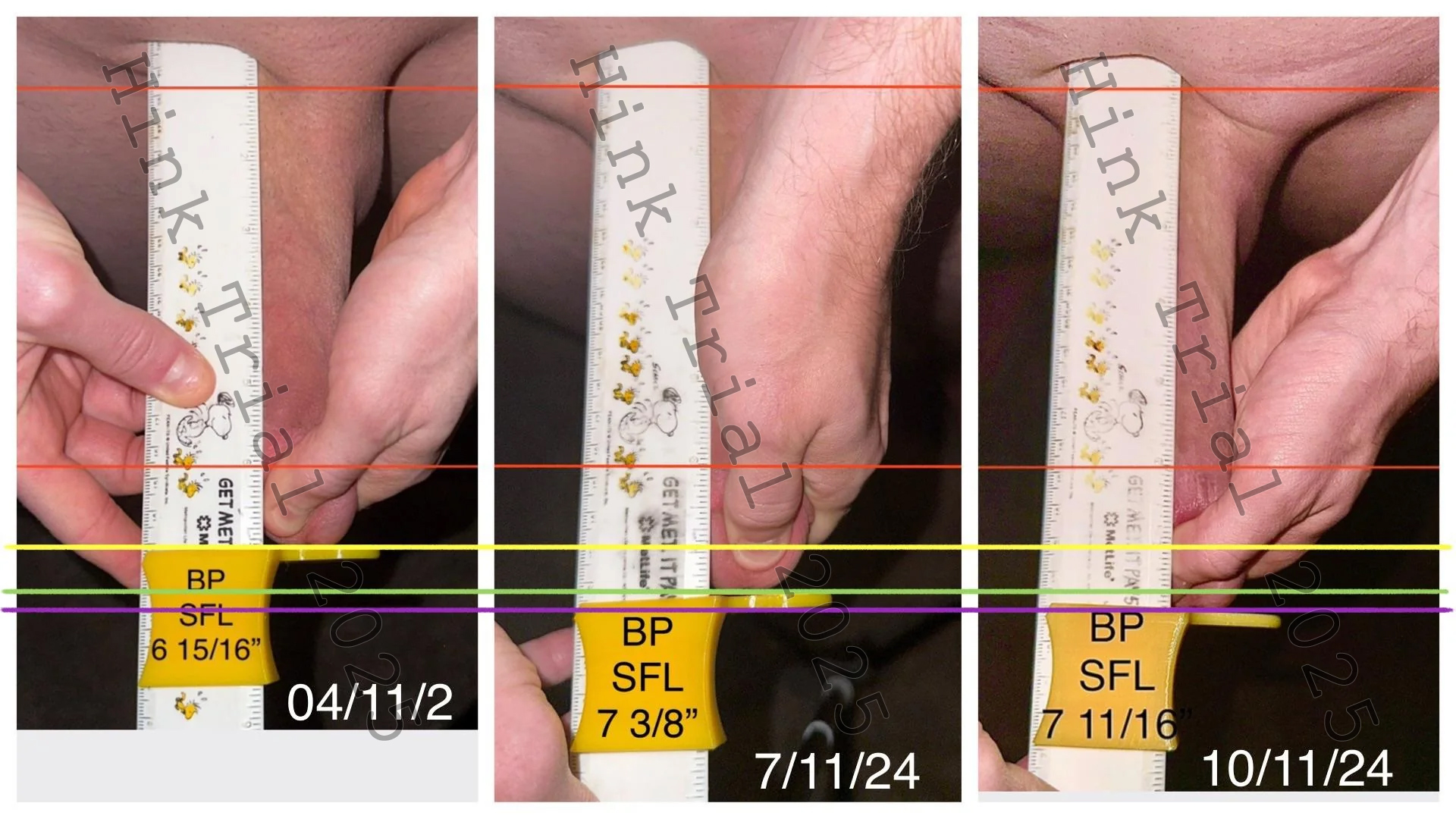
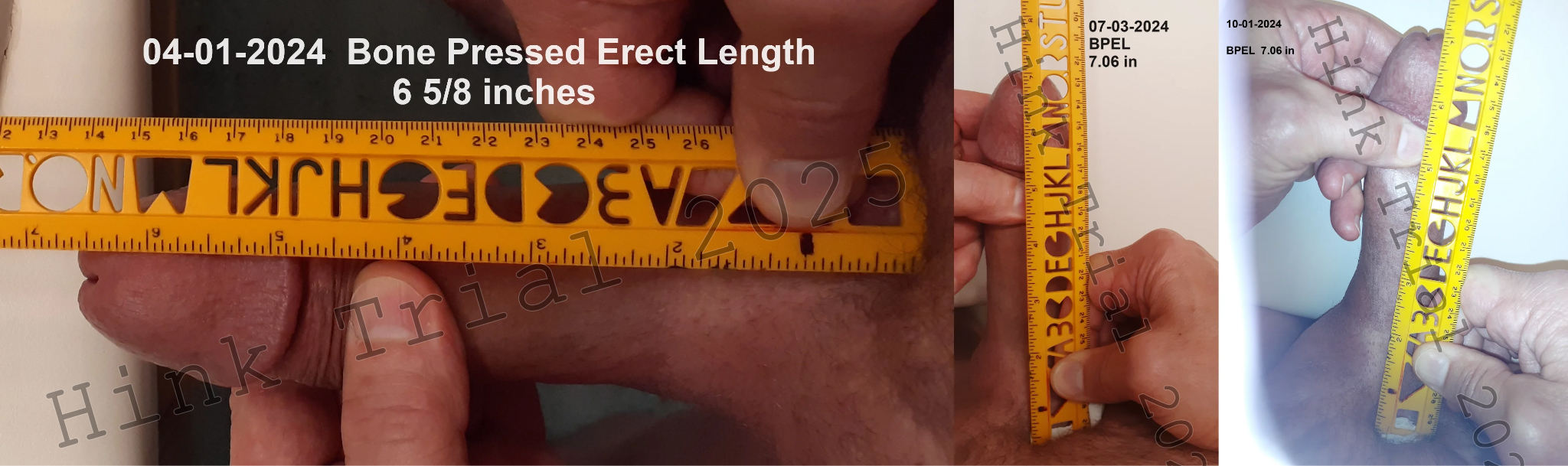
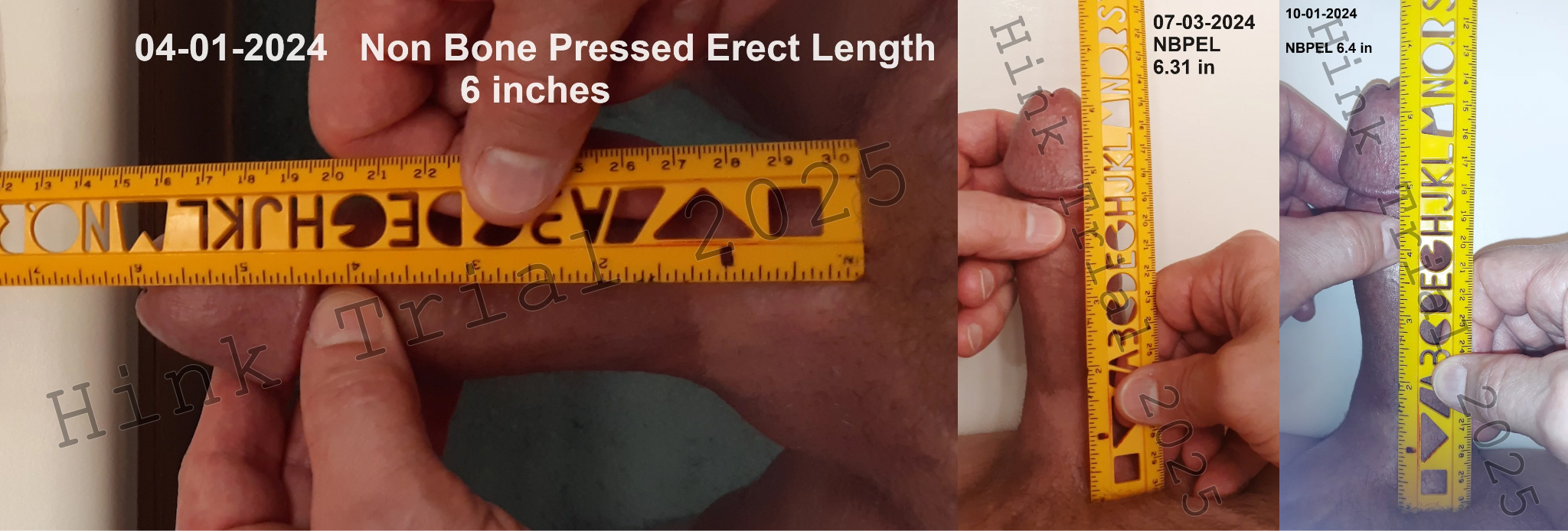
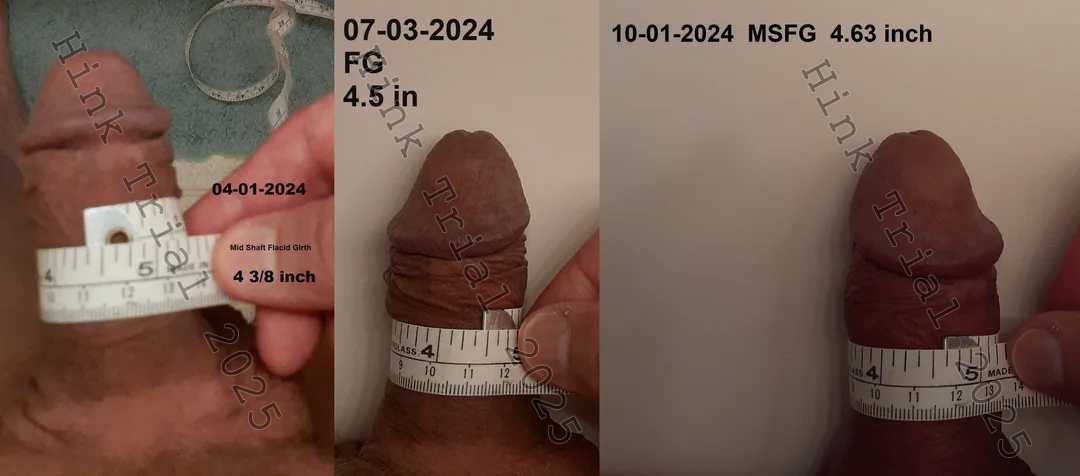
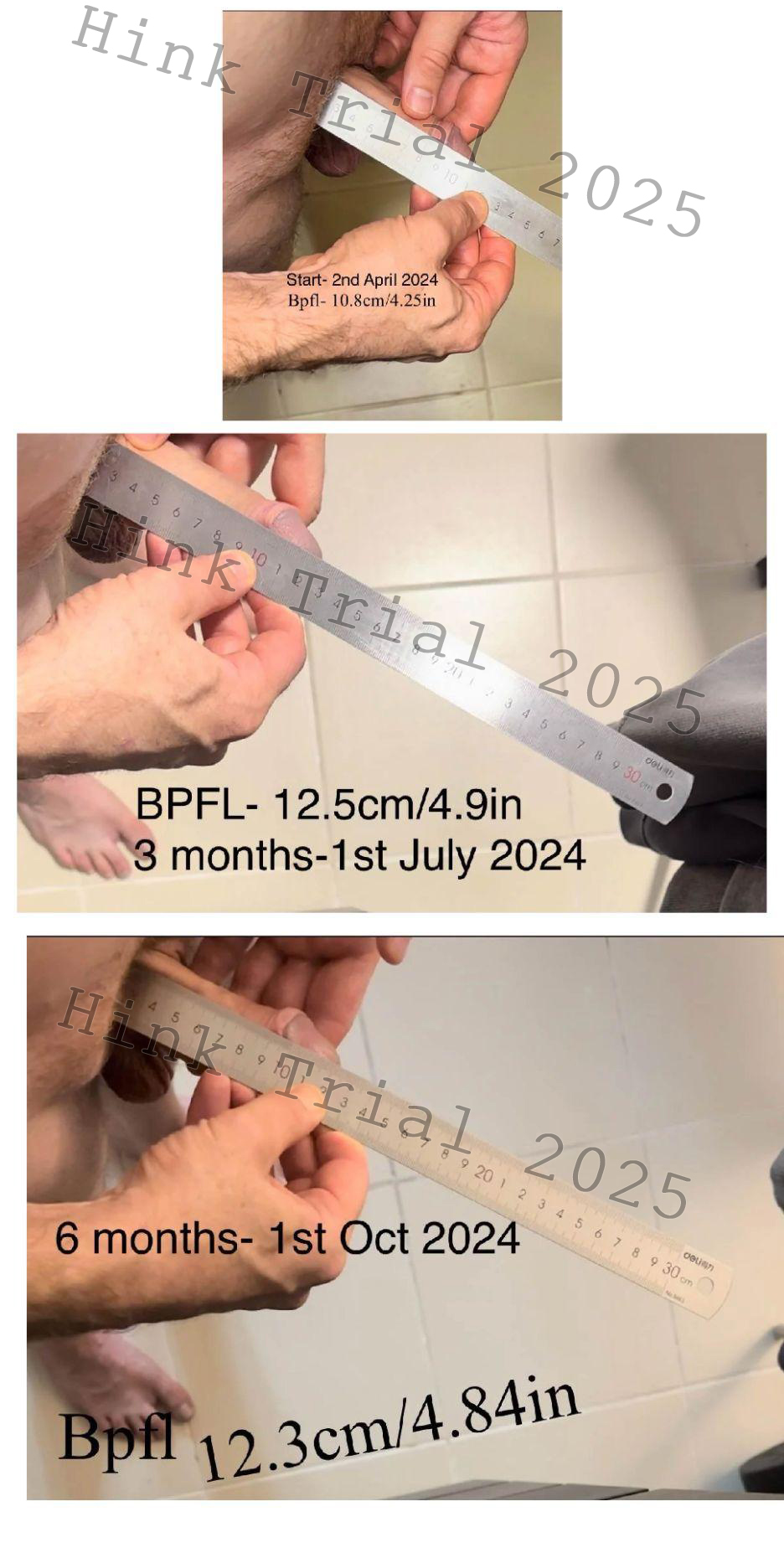
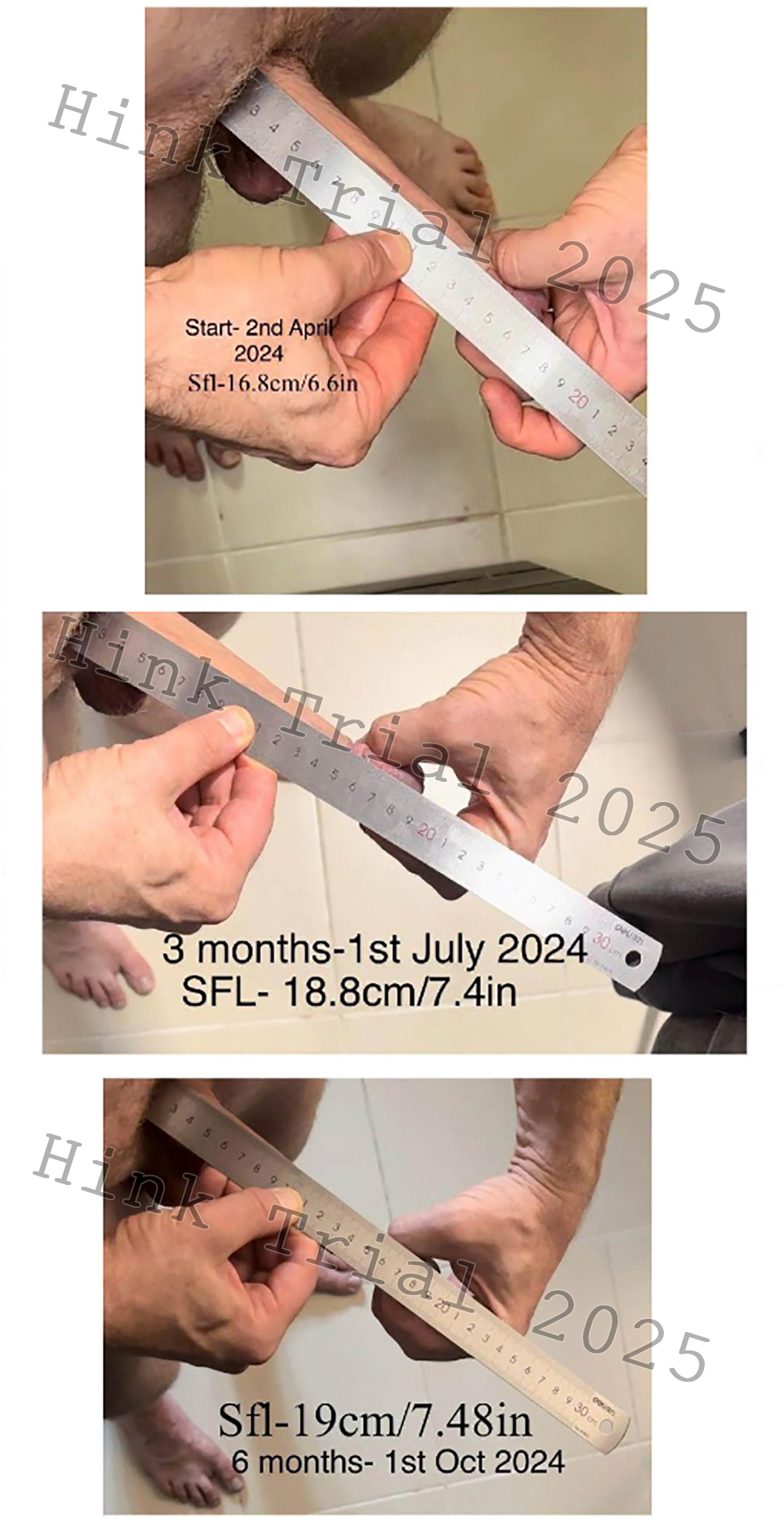
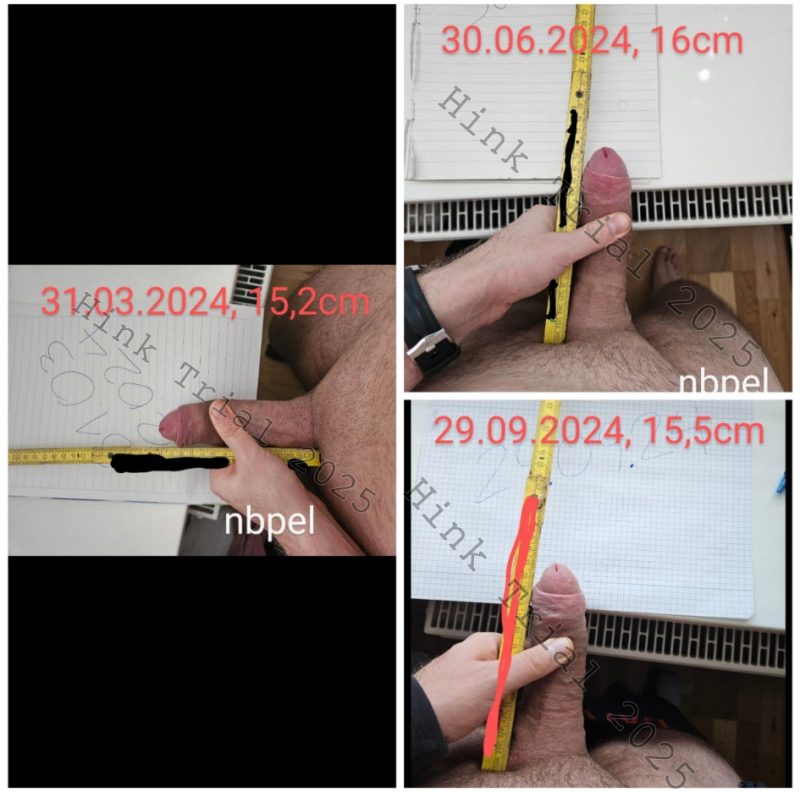
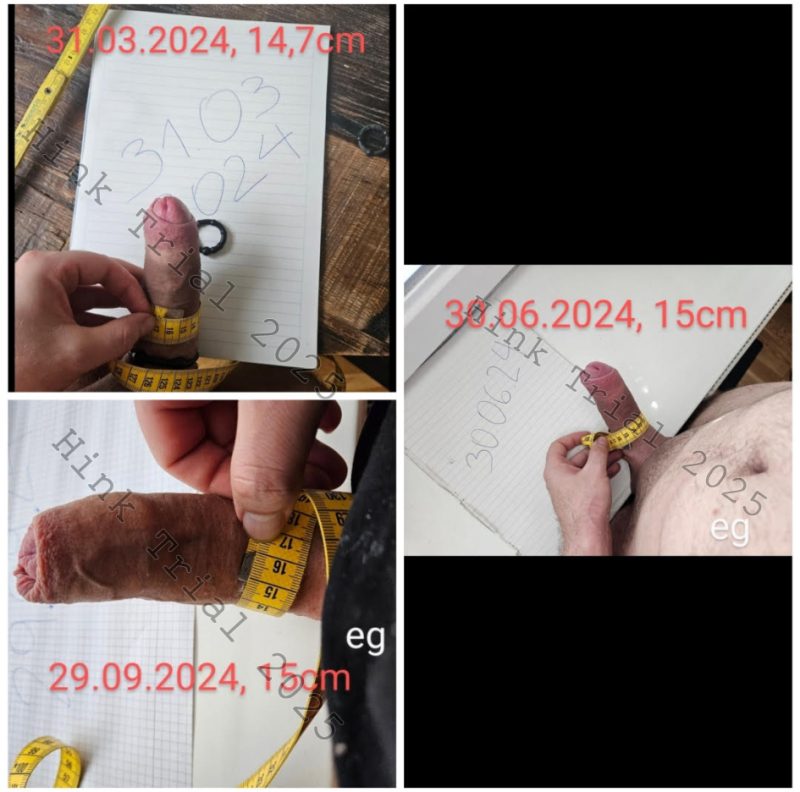
Photographic Evidence
Participant 1

Participant 2


Participant 3
Participant 4




Participant 5


Participant 6
Participant 7